Section Abstract Introduction Methods Results Discussion Conflict of Interest Acknowledgment References
Clinical Research
Basal follicle stimulating hormone and leptin on the day of hCG administration predict successful fertilization in in vitro fertilization
pISSN: 0853-1773 • eISSN: 2252-8083
http://dx.doi.org/10.13181/mji.v25i1.1215 Med J Indones. 2016;25:39–43
Received: March 09, 2015
Accepted: February 08, 2016
Author affiliation:
Department of Obstetrics and Gynaecology, Faculty of Medicine, Universitas Indonesia, Cipto Mangunkusumo Hospital, Jakarta, Indonesia
Corresponding author:
Andon Hestiantoro
E-mail: hestiantoro@gmail.com
Background
Successful pregnancy in in vitro fertilization (IVF) program depends on multiple factors. This study aimed to determine whether age, body mass index (BMI), basal follicle stimulating hormone (FSH), estradiol, and leptin on the day of trigger ovulation with human chorionic gonadotropin (hCG) might be used as predictor for successful oocyte fertilization in in vitro fertilization (IVF) program.
Methods
This is a cross sectional study conducted in Yasmin Fertility Clinic, Cipto Mangunkusumo Hospital, Jakarta, Indonesia. Forty participating patients underwent IVF program, excluding smokers, patients with diabetic, morbid obesity, and severe oligospermia or azoospermia. Age, BMI, basal FSH, estradiol, leptin on the day of hCG administration, oocyte count on oocyte retrieval, the number of mature oocyte, and fertility rate were analyzed using bivariate and multivariate analysis to determine which eligible factors play role in predicting the successful of fertilization.
Results
Significant correlation was found between basal FSH level and serum leptin/oocyte ratio on the day of hCG administration with successful fertilization. We found probability formula as follows: 1/(1+exp –(6.2 - 0.4(leptin serum/ oocyte ratio) - 0.8(basal FSH)), with 77.8% sensitivity, 77.8% specificity, and AUC levels of 85.6% indicating strong predictability. Probability of successful fertilization related to basal FSH level of 5.90 mIU/mL and leptin serum/oocyte ratio of 3.98.
Conclusion
The formula consisting of basal FSH and leptin serum/oocyte ratio on the day of trigger ovulation was capable in predicting the probability of successful fertilization in IVF procedure.
Keywords
basal FSH, IVF, leptin serum, oocyte ratio
As a modality for managing infertility problems, in vitro fertilization (IVF) program has still shown low success rate of 30–40%.(1) Successful pregnancy in IVF program depends on the age of subject, etiological factors, duration of infertility, and endometrial receptivity. Others are associated with the types of treatment, such as intra-cytoplasmic sperm injection (ICSI), frozen embryo, the number of oocytes recovered, and the quality of transferred embryos.1 The quality of transferred embryo plays an important role with IVF success, and it is related to pre embryo or two pro nucleus (2pn) cell. Successful fertilization showed fertilization rate of 2pn cells is more than 65%.2
The quality of oocytes plays a key role in a proper embryo development. The competence of oocytes depends on numerous processes taking place during the whole oogenesis, which are age, body mass index (BMI), basal follicle stimulating hormone (FSH), and estradiol.3 Estradiol production will increase along the follicle size growing and the oocyte become more mature. Hence, the higher level of estradiol could be the characteristic of oocyte maturation. Despite of being the general marker of oocyte maturation, estradiol still could not be the predictor of cytoplasm maturation since there was no different result observed in estradiol levels of follicular fluid between fertilized and unfertilized oocytes.4
Recent studies have suggested that leptin receptor (Ob-R) can mediate signal through either the mitogen activated-protein kinase (MAPK) or the Janus-activated kinase/signal transducer and activator of transcription signal-transduction pathway. The role of leptin has proven in both nuclear and cytoplasmic maturation. During oocyte maturation, phosphorylated-MAPK content was increased by leptin, and leptinstimulated oocyte maturation was blocked when a specific MAPK activation inhibitor suppressed leptin-induced MAPK phosphorylation. It is demonstrating the leptin enhanced nuclear maturation via activation of the MAPK pathway.4
Leptin was considered to be one of the oocyte maturation predictor by looking at the activation of the MAPK and the maturation promoting factors (MPF). Along with age, BMI, basal FSH and estradiol, leptin is another important factor in predicting fertilization rate in IVF. In addition, the most important key of successful fertilization is not only limited to the follicle size, but precisely the final step, which is the oocyte maturation degree assessed from the cumulus mass expansion and the density of corona cell around the oocyte.4 In IVF cycles, hCG administration is used as a surrogate luteinizing hormone (LH) surge to induce development and maturation of larger ovarian follicles (≥15 mm in diameter) that have acquired granulose cell LH/hCG receptors.5,6 For this reason, leptin serum level is needed to be examined around the time when predicted oocyte maturation occurs, which is in the day of hCG administration for oocyte maturation. In addition, since maturation of each oocyte was being assessed, leptin level in each follicle was obtained by measuring the ratio of leptin serum level with oocyte count.
As it is important to identify the marker for determining oocyte maturation, this study aimed for determining the suitability of leptin serum on the day of human chorionic gonadotropin (hCG) administration as the predictor for successful oocyte fertilization in IVF program, while assessed the association between age, BMI, basal FSH, follicular estradiol, and leptin serum with success rate of fertilization in IVF program.
METHODS
This was a cross sectional study conducted in Yasmin Fertility Clinic, Cipto Mangunkusumo Hospital, Jakarta, Indonesia, from August 2008 to May 2009. The samples were 40 subjects. Subjects were chosen according to inclusion and exclusion criteria. The inclusion criteria was patient underwent IVF program, while the exclusion criteria were smokers, diabetes mellitus, morbid obesity, and severe oligoospermia or azoospermia. The protocol of this study has been approved by Medical Ethics Committee of Universitas Indonesia (No. 27/PT02.FK/ETIK/2009).
Subjects underwent interview, physical examination, and laboratory examination. About 5 mL of venous blood were taken for day three basal FSH and later on oocyte retrieval for serum estradiol and serum leptin. Leptin serum was obtained on the day of hCG administration. Leptin serum per oocyte ratio was measured by dividing leptin serum on the day of hCG administration with numbers of oocyte during oocyte retrieval.
Subjects’ ages were obtained in anamnesis, while BMI was calculated from the weight and height obtained using a weight scale. FSH level was measured in the third day of menstruation; preovulation estradiol level was measured before hCG administration, and leptin serum level was measured in the day of hCG administration. Those variables were obtained from laboratory data of the venous puncture analysis. Successful fertilization rate defined as the occurring of more than 65% fertilization according to the laboratory data.
Pre-embryo results were recorded as data and processed with SPSS for Windows v.13. Bivariate analysis using T-test and Mann-Whitney test were performed to the factors affecting oocyte fertilization, continued with multivariate analysis using logistic regression.
RESULTS
Bivariate analysis on fertilization success
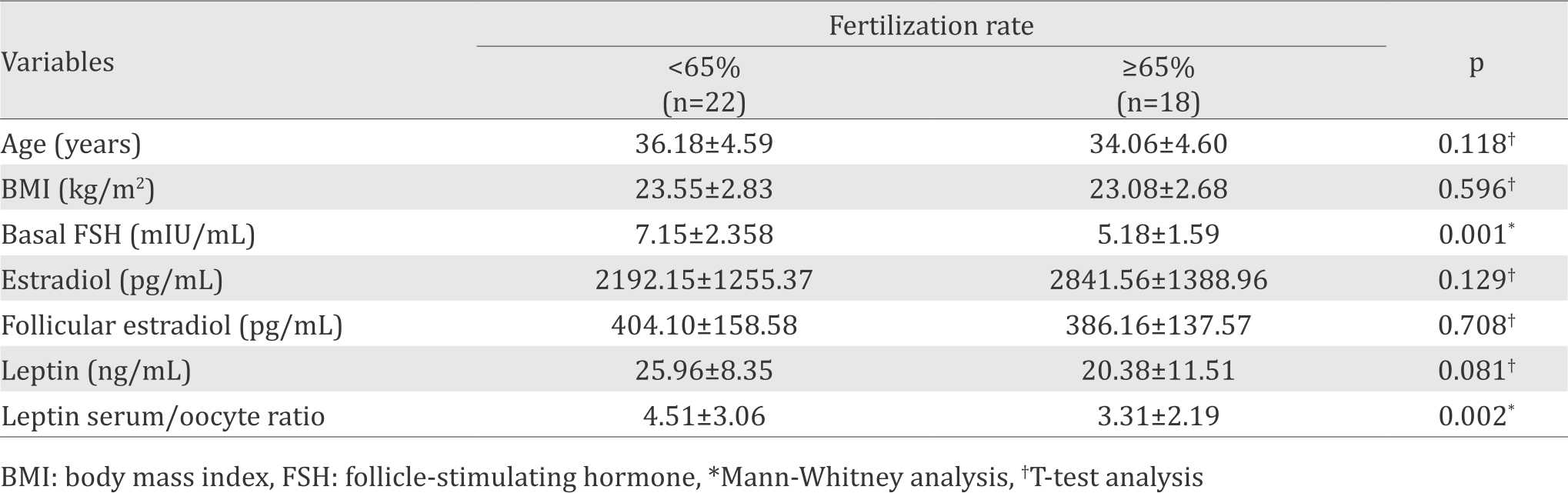
There were 40 subjects aged 26–44 years old recruited in this study. They were divided into two groups: (1) group with fertilization rate <65%, which considered as not successful; (2) group with fertilization rate ≥65%, which considered as successful. The numbers and demographic characteristic including age and BMI of both groups were similar with the average age about 35 years and the average BMI about 23 kg/m2.
Bivariate analysis was conducted between two groups. T-test analysis was performed to age, BMI, estradiol on hCG-administration day, leptin serum on hCG-administration day, and follicular estradiol on hCG-administration day. Mann- Whitney analysis was performed to basal FSH and leptin serum. The success of fertilization procedure is related to basal FSH and leptin serum significantly with p value of 0.001 and 0.002 respectively (Table 1).
Table 1. Factors affecting fertilization success
Multivariate analysis on fertilization success
Multivariate analysis with logistic regression was performed on age, basal FSH, estradiol on hCG-administration day, leptin serum on hCGadministration day, and leptin serum. From the logistic regression, we found the variables related to success fertilization are basal FSH and leptin serum (Table 2).
Table 2. Logistic regression on basal FSH, estradiol on the day of hCG administration, leptin on the day of hCG administration, and leptin per oocyte ratio on the day of hCG administration
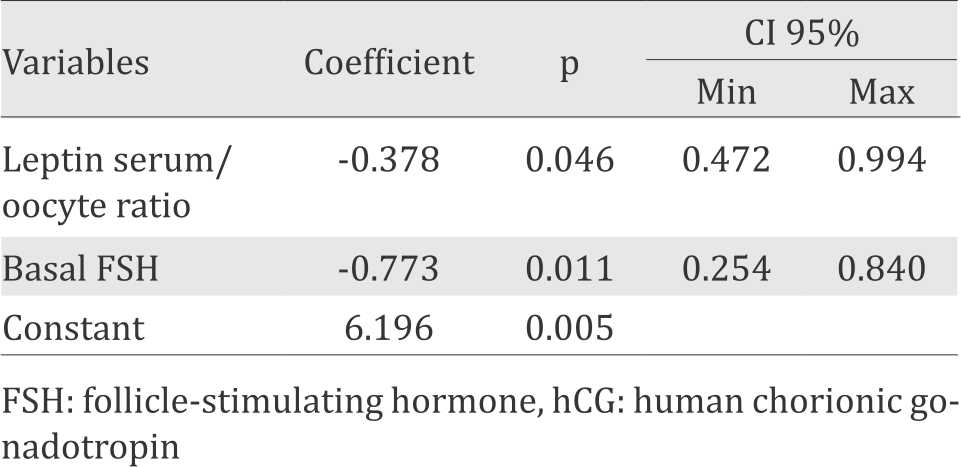
In counting the probability of the success in fertilization procedure, those factors then were included in the following equation:
Probability = 1/(1+exp –[6.2 - 0.4(leptin serum/oocyte ratio) -0.8(basal FSH)])
An example of a case using this equation is provided as follows:
Basal FSH = 4.80 mIU/mL; leptin serum hCG day
administration = 16 ng/mL; oocyte=5
Leptin serum/oocyte ratio: 16/5=3.20
Y = 6.2–(0.4x3.2)–(0.8x4.8)= 1.3
Probability = 1/(1 + exp–1.3)= 0.78
It can be concluded that the basal FSH of 4.80 mIU/mL and leptin serum per oocyte ratio of 3.20 has probability for successful fertilization as much as 78%.
From the equation above, receiver operating characteristic (ROC) curve was analyzed to find out the sensitivity and specificity of the equation. The ROC curve has area under curve (AUC) of 85.6%, which statistical interpretation showing 80%-90% as strong predictability (Figure 1).
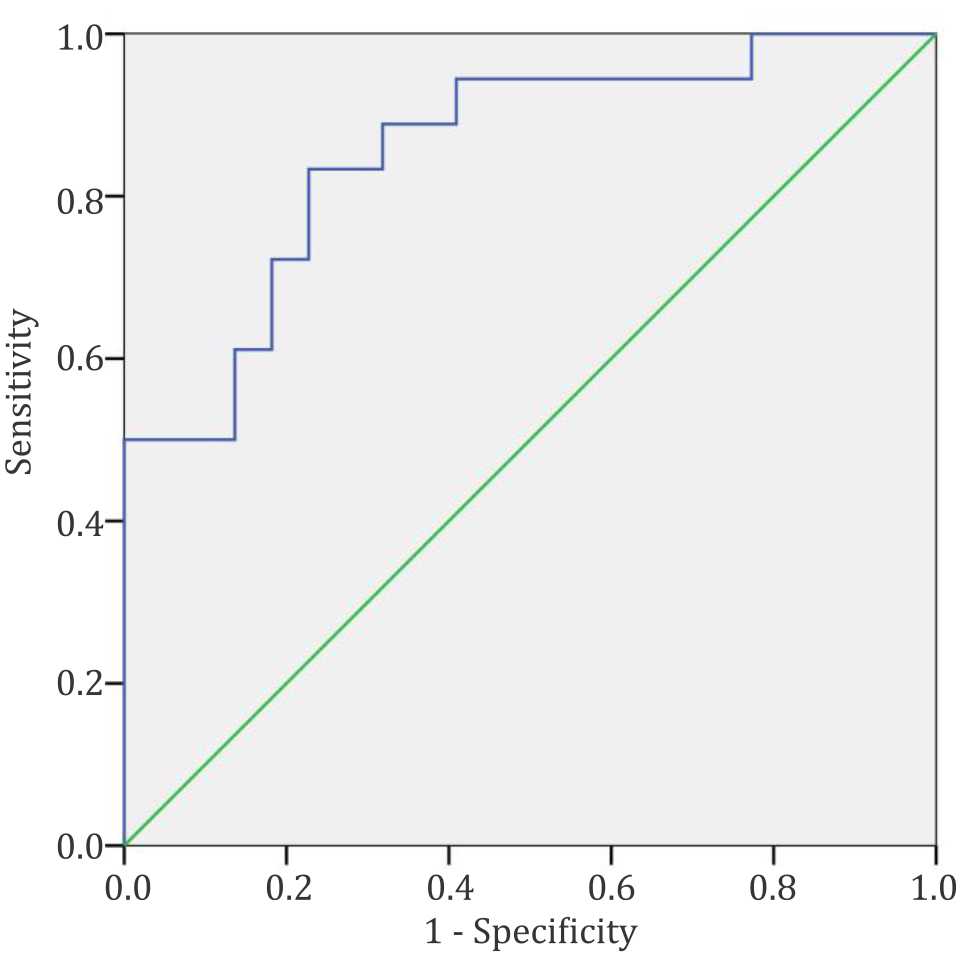
Figure 1. Receiver operating characteristic (ROC) curve containing basal FSH and leptin serum role in predicting the success of fertilization
The AUC is 85.6% concluded as strong predictability, with 77.8% sensitivity and 77.8% specificity. The sensitivity and specificity were found on probability value of 0.474, which means probability level above 0.474 has successful fertilization predictability. Maximum level of basal FSH is 5.90 mIU/mL and the leptin serum is 3.98.
DISCUSSION
The role of basal FSH as fertilization success predictor
In this study, successful fertilization was marked by fertilization rate ≥65%. We found lower basal FSH (5.18 mIU/mL vs 7.15 mIU/mL, p=0.001) in successful fertilization. From the previous study, Andersen et al7 reported that supraphysiological FSH level affected oocyte viability in assisted reproductive technology. The regulation of progesterone production by the developing follicles during controlled ovarian stimulation is a complicated interplay of hormonal systems involving the theca and granulosa cells, and the effect of the actions of both LH and FSH7 It has been reported that pregnancy rate will reduce significantly if day three FSH levels were more than 15 mIU/mL. Very few pregnancy achieved if day three FSH levels were more than 25 mIU/mL.8 Another study showed FSH level of 6.5–15 mIU/mL as poor responders.9 Basal FSH level performed better as a sole prognosticator for treatment failure, but the high cut off level necessary to reach sufficient prognostic power inevitably reduces the number of patients that may benefit from the test. Basal FSH is a limited value in the prediction of pregnancy rate after IVF and should only be applied if clear consequences, therefore another predictive factor is needed to predict fertility success.10
The role of leptin as predictor for fertilization
We found lower leptin level (20.38 ng/mL vs 25.96 ng/mL, p=0.081) and lower leptin serum (3.31 vs 4.51, p=0.002) in successful fertilization. Leptin enhances MAPK fosforilation and cyclin B1 expression, which oocyte maturation occurs.4 In fact, higher leptin level reduces oocyte maturation. Anifandis et al11 has conducted prospective studies to assess prognostic value of leptin on embryo quality. Increased leptin level above 59.48±7.6 ng/mL related to bad embryo quality and leptin level above 56.87±5.52 ng/ mL related to pregnancy failure. Higher leptin level related to decreased ovarian stimulation, follicular maturation, embryo quality, and pregnancy success. Mantzoros et al12 showed that lower leptin level is a pregnancy predictive factor in normal woman, even in polycystic ovarian syndrome (PCOS) patients.
Predictor model for fertilization in IVF
The model pointed out that the lower basal FSH level and leptin serum will have higher fertilization success, and even then lowest level of both variables could not be determined yet. This is the same with other studies that showed lower basal FSH and leptin have higher probability of oocyte maturation and embryonic development until pregnancy outcome. There is still no study that put basal FSH together with leptin serum to predict fertilization. It was previously mentioned by Bancsi et al10 that basal FSH levels were quite limited in predicting on going pregnancy rates after IVF. Previous studies on leptin as the predictor of IVF success showed that higher leptin reduced embryo development and pregnancy rate.11,12 This study found that the formulation consisting of basal FSH and leptin per oocyte ratio combination can be good in predicting the probability for successful fertilization.
Clinical importance of the equation above is that we can predict the success of fertilization process, decide which patient has the best response, help in counseling of the patient, and finally would became prognostic factors affecting the success of fertilization process, and raise the efficiency in IVF.
The level of basal FSH and leptin serum per oocyte ratio
We found the maximum level of basal FSH is 5.90 mIU/mL and leptin serum per oocyte ratio is 3.98. The minimum level of both variables could no be determined yet by this study. The count of basal FSH is the same with other studies, but the count of leptin serum per oocyte ratio is a new finding in this study.
In conclusion, this study had found correlation between basal FSH and leptin serum with successful fertilization. The formulation found, which consisted of basal FSH and leptin serum/ oocyte ratio, was capable of predicting the probability of successful fertilization in IVF procedure. This correlation between basal FSH and leptin serum was observed as success value for oocyte fertilization process
Conflicts of Interest
The authors affirm no conflict of interest in this study.
Acknowledgment
The authors express their gratitude to the team of Yasmin Fertility Clinic, Jakarta, for being very helpful in producing this study, and Amalia Shadrina, MD for her effort in making this paper complete.
REFERENCES
- Toma´s C, Tikkinen K, Tuomivaara L, S.Tapanainen J, Martikainen H. The degree of difficulty of embryo transfer is an independent factor for predicting pregnancy. Hum Reprod. 2002;17(10):2632–5.
- Practice Committee of Society for Assisted Reproductive T, Practice Committee of American Society for Reproductive Medicine. Guidelines on number of embryos transferred. Fertil Steril. 2008;90(5 Suppl):S163–4.
- Marteil G, Richard-Parpaillon L, Kubiak JZ. Role of oocyte quality in meiotic maturation and embryonic development. Reprod Biol. 2009;9(3):203–24.
- Craig J, Zhu H, Dyce PW, Petrik J, Li J. Leptin enhances oocyte nuclear and cytoplasmic maturation via the mitogen-activated protein kinase pathway. Endocrinology. 2004;145(11):5355–63.
- Matorras R, Meabe A, Mendoza R, Prieto B, Ramon O, Mugica J, et al. Human chorionic gonadotropin (hCG) plasma levels at oocyte retrieval and IVF outcomes. Journal of assisted reproduction and genetics. 2012;29(10):1067–71.
- Beretsos P, Partsinevelos GA, Arabatzi E, Drakakis P, Mavrogianni D, Anagnostou E, et al. “hCG priming” effect in controlled ovarian stimulation through a long protocol. Reprod Biol Endocrinol. 2009;7:91.
- Andersen CY, Ezcurra D. Human steroidogenesis: implications for controlled ovarian stimulation with exogenous gonadotropins. Reprod Biol Endocrinol. 2014;12:128.
- Excellence NIfC. Fertility: assessment and treatment for people with fertility problems. London: RCOG Press; 2004.
- Patrizio P, Vaiarelli A, Levi Setti PE, Tobler KJ, Shoham G, Leong M, et al. How to define, diagnose and treat poor responders? Responses from a worldwide survey of IVF clinics. Reprod Biomed Online. 2015;30(6):581–92.
- Bancsi LF, Huijs AM, den Ouden CT, Broekmans FJ, Looman CW, Blankenstein MA, et al. Basal folliclestimulating hormone levels are of limited value in predicting ongoing pregnancy rates after in vitro fertilization. Fertil Steril. 2000;73(3):552–7.
- Anifandis G, Koutselini E, Stefanidis I, Liakopoulos V, Leivaditis C, Mantzavinos T, et al. Serum and follicular fluid leptin levels are correlated with human embryo quality. Reproduction. 2005;130(6):917–21.
- Mantzoros CS, Cramer DW, Liberman RF, Barbieri RL. Predictive value of serum and follicular fluid leptin concentratrions during assisted reproductive cycles in normal women and in women with the polycyistics ovarian syndrome. Hum Reprod. 2000;15(3):539–44.
Copyright @ 2016 Authors. This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original author and source are properly cited.
mji.ui.ac.id