Case Report
Endoscopic incision of protruding right ureterocele in a single collecting system: a case report
pISSN: 0853-1773 • eISSN: 2252-8083
http://dx.doi.org/10.13181/mji.v25i4.1352 Med J Indones. 2016;25:240–4
Received: January 12, 2016
Accepted: November 01, 2016
Author affiliation:
Department of Urology, Faculty of Medicine, Universitas Indonesia, Cipto Mangunkusumo Hospital, Jakarta, Indonesia
Corresponding author:
Harrina E. Rahardjo
E-mail: harrinaerlianti@yahoo.com
Protruding ureterocele is a very rare case found in the literature. We are reporting a 21 year-old female with an intermittent protruding mass from urethra, accompanied by dysuria, hematuria, and recurrent urinary tract infection. Inspection of the external genitalia revealed a protruding mass from the urethra which could be reduced manually. Excretory urography showed bilateral single collecting systems, grade II hydronephrosis of the right kidney, and a cobra head appearance of the lower right pelvis. The patient was diagnosed with a protruding right ureterocele in a single collecting system, and thus, endoscopic incision of a ureterocele was performed. Ultrasonography which was carried out three weeks after the procedure confirmed no residual hydronephrosis or ureterocele in the bladder. Voiding cystourethrography (VCUG) underwent at a threemonth- follow up revealed a grade 5 vesico-ureteral reflux (VUR) on the right side. Surgical reimplantation was then considered. In conclusion, endoscopic incision was safe and yielded good result for protruding ureteroceles, but the need for secondary surgery in several conditions should be considered.
Keywords
endoscopic incision, protruding ureterocele
A ureterocele is a cystic dilatation of the distal ureter.1 It has been proposed that incomplete dissolution of the Chwelle’s membrane is the embryological basis for ureterocele formation.2,3 Ureteroceles can be further classified as intravesical or extravesical. Intravesical ureteroceles (orthotopic) are entirely located within the bladder and above the bladder neck, while extravesical ureteroceles (ectopic) are partially located at the bladder neck or urethra.1,2 Ureteroceles can also be presented with a double collecting system (duplex system ureterocele) or a single collecting system (single system ureterocele).1,3,4
The incidence of ureteroceles is around 1:4,000 children and is 4–7 times more frequently found in female.2,3 At the moment, there is no epidemiological data for ureteroceles in South East Asia or in adult population. Ureteroceles are mostly associated with upper pole moiety in double collecting systems (~80%), but a small percentage of ureteroceles (~20%) can be found in single systems.1,3,4
Ureteroceles may exhibit varying symptoms from urinary tract infection, obstruction to incontinence, and it may even protrude out of the urethra. Protruding ureteroceles have been reported, but are rarely found in the literature. Ureteroceles can be managed with several modalities, including a minimal invasive endoscopic incision. We are reporting a protruding orthotopic ureterocele in an adult female with a single collecting system, which was successfully treated with an endoscopic incision.
CASE REPORT
A 21 year-old female came to our hospital with a protruding mass from the urethra. She has experienced this condition since she was 12 years old. The patient also complained of dysuria, hematuria, and recurrent urinary tract infection. There was no history of trauma, flank pain, vaginal birth, or previous gynecological/urological surgery. On the physical examination, inspection of the external genitalia revealed a protruding mass from the external urethral orifice with a round shape, bright brown-red color, cystic consistency, smooth surface, and a size of 3x2x2 cm. It could be reduced manually back through the urethra. Ultrasonography of the upper urinary tract showed a mild hydronephrosis of the right kidney. Excretory urography revealed bilateral single collecting systems, grade II hydronephrosis of the right kidney, and a cobra head appearance of the lower right pelvis. A urinary tract infection was evident from urine analysis. Other laboratory results were unremarkable.
The patient was then diagnosed with a protruding right ureterocele in a single collecting system. Therefore, an endoscopic incision of the ureterocele was performed. The patient was discharged one day after the procedure with continued oral antibiotic and analgesia. At a three-week-follow up, urinalysis of the patient who had dysuria revealed urinary tract infection which was then resolved by antibiotic. There was no residual hydronephrosis of the right kidney or ureterocele in the bladder on ultrasound examination performed three weeks after the procedure. Voiding cystourethrography (VCUG) was done at the third month and a grade 5 vesicoureteral reflux (VUR) on the right side was observed. The patient was scheduled for ureteral reimplantation. However, she decided to postpone the surgery due to the lack of complaints.
DISCUSSION
Patients with ureterocele may have varying presenting symptoms such as urinary tract infection, obstruction, or incontinence.2,6 There are several reported cases in the literature on protruding ureteroceles through the urethra, but they are very rare, as first reported by Sen et al.12 In children, the exact incidence of protruding ureteroceles is unknown, but it has been reported to be less than five percent.7 In adults, the exact number of incidence is also unknown, with no more than five cases reported in the last ten years. Such urethral prolapse may be caused by weakness of the urethral wall distal to the ureterocele.8 Our patient experienced a protruding mass from the urethra with a history of intermittent dysuria, hematuria, and recurrent urinary tract infection. The mass had a smooth round shape with bright brown-red color, and it could still be reduced back through the urethra, suggesting a diagnosis of a protruding ureterocele.9 The abscence of history of flank pain might indicate there was no severe urinary tract obstruction or upper urinary tract infection.
A diagnosis of a protruding ureterocele can further be confirmed by the presence of a ureterocele in bladder through radiologic imaging. Excretory urography and ultrasonography have been widely used to reveal ureteroceles.2,4 Excretory urography can identify the duplication of urinary tract, urinary tract obstruction, and ureterocele itself (as a cystic dilatation in the bladder).4 Voiding cystourethrography and renal scanning can also be performed to evaluate reflux and split renal function.2
Our patient’s excretory urogram showed a bilateral single collecting system and a cobra head appearance suggestive of a ureterocele on the right side (Figure 1). A hydronephrosis of the right kidney was also observed using ultrasonography, suggestive of an obstruction caused by the ureterocele. Based on physical and radiologic examination, we confirmed the patient’s diagnosis of a protruding right ureterocele in a single collecting system. Single system ureteroceles in adults are very rare and usually associated with preserved ipsilateral renal function and minimal hydronephrosis. It may occasionally be complicated with calculus formation, which was not found in our patient.4,5
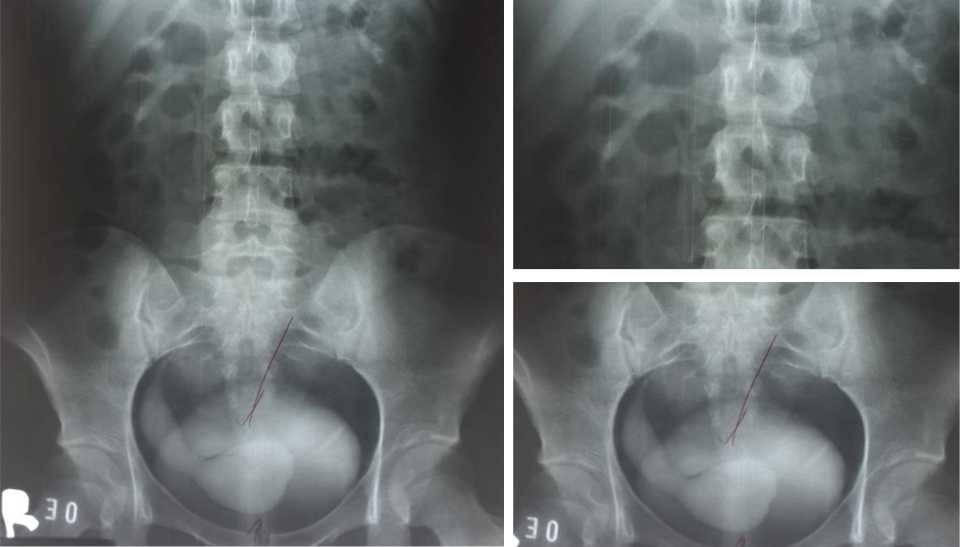
Figure 1. Excretory urogram revealing hydronephrosis of the right kidney and a “cobra head” appearance of the right vesical junction area
Management of ureteroceles should be oriented toward symptoms improvement and preservation of renal function.3,10,11 Several modalities include conservative approach, endoscopic decompression, ureteral reimplantation, partial nephroureterectomy, or complete primary reconstruction. The choice of management should depend on patient’s clinical status, age, renal function, presence of reflux or obstruction, presence of double or single collecting system, ectopic or orthotopic ureterocele, and the preferences of the patient and the surgeon.3,11
In our patient, endoscopic incision of the ureterocele was performed to decompress the ureterocele and to release the obstruction (Figure 2). In several studies, endoscopic incisions have been reported to yield good result in terms of safety and symptoms or ureterocele resolution.10,11 Three cases reported by Scovell et al,5 Sen et al,12 and Westesson13 also showed the success of endoscopic management of ureteroceles. In our case, at a three-weekfollow up, there was no residual hydronephrosis or ureterocele found from ultrasonography, indicating resolution of the disease (Figure 3).
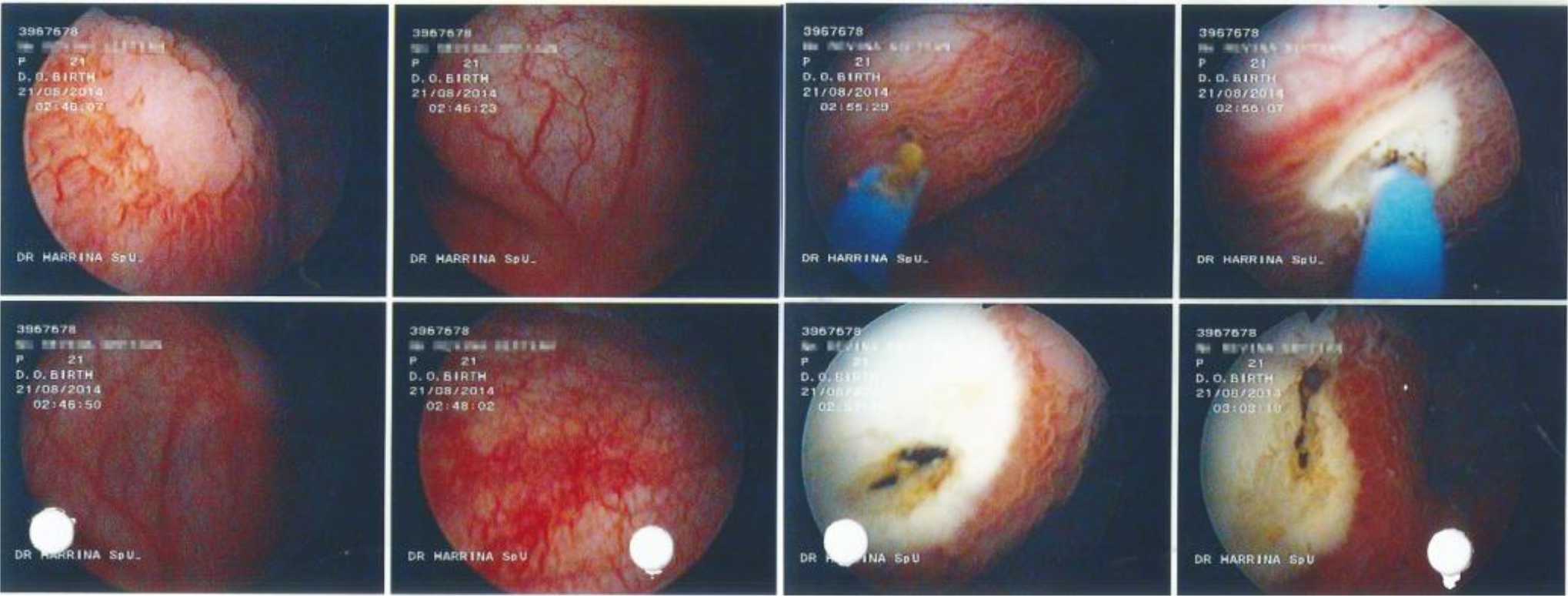
Figure 2. Endoscopic incisionn of the ureterocele

Figure 3. Ultrasonography at a three-week-follow up
Endoscopic incision of ureteroceles might result in VUR in some patients, with varying reports of incidence (0–32%). Therefore, VCUG was performed three months after the endoscopic incision.10 Secondary surgery is necessary when the decompression is not effective, significant reflux is found, or when there is significant obstruction.3,11 In our patient, significant vesicoureteral reflux (grade 5) was found on the right side (Figure 4), indicating a need for a secondary surgery. Reimplantation of the ureter was then scheduled. We would expect a good prognosis for our patient because the procedure is generally safe and provides excellent success rates (92–98%) in such case.3
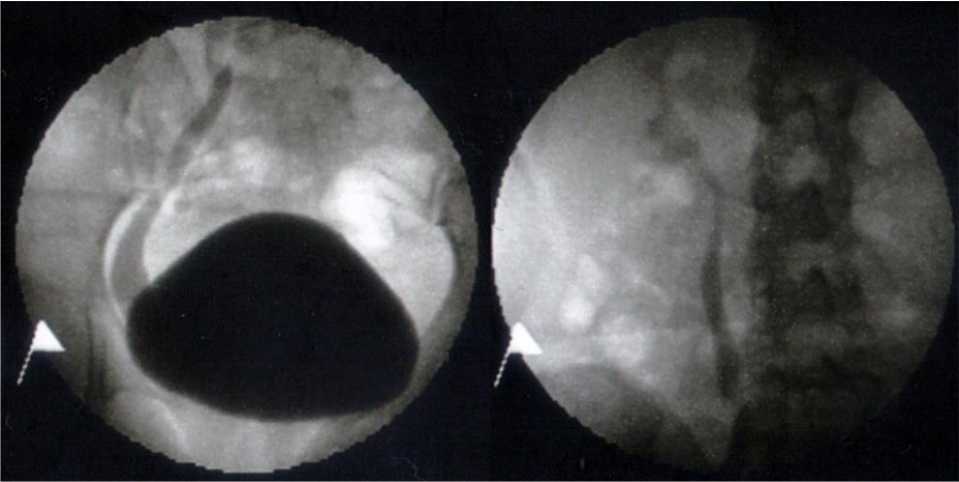
Figure 4. Voiding cystourethrogram at a three-monthfollow up revealed reflux of the right ureter
In conclusion, ureteroceles may exhibit varying symptoms and may even protrude out of the urethra. While several modalities up to open surgery can be selected, endoscopic approach can be used and has been reported to be safe and yield good results in the management of ureteroceles.
Conflicts of Interest
The authors confirm no conflict of interest in this study.
Acknowledgment
None.
REFERENCES
- Peters CA, Schlussel RN, Mendelsohn C. Ectopic ureter, ureterocele, and ureteral anomalies. In: Kavoussi LR, Novick AC, Partin AW, Peters CA, editors. Campbell- Walsh urology. 10th ed. Philadelphia: Elsevier Saunders; 2012. p. 3236–60.
- Kogan BA. Disorders of the ureter & ureteropelvic junction. In: Tanagho EA, McAninch JW, editors. Smith’s general urology. 17th ed. New York: McGraw-Hill; 2008. p. 560–2.
- Tekgül S, Dogan HS, Erdem E, Hoebeke P, Kočvara R, Nijman JM, et al. Guidelines on paediatric urology. Eur Assoc Urol. 2014. p.90–4.
- Zerin JM, Baker DR, Casale JA. Single-system ureteroceles in infants and children: imaging features. Pediatr Radiol. 2000;30(3):139–46.
- Scovell JM, Chan RC, Khavari R. Prolapse of a single system large ureterocele containing multiple stones in a pregnant woman. Urology. 2014;83(3):e3–4.
- Muhammed A, Hussaini MY, Ahmad B, Hyacinth MN, Garba KD. Ureteroceles in adults: management of patients in Zaria, Nigeria. Arch Int Surg. 2012;2(1):24–8.
- Ilica AT, Kocaoğlu M, Bulakbaşi N, Sürer I, Tayfun C. Prolapsing ectopic ureterocele presenting as a vulval mass in a newborn girl. Diagn Interv Radiol. 2008;14(1):33–4.
- Konami T, Wakabayashi Y, Takeuchi H, Tomoyoshi T. Female wide urethra masquerading as a urethral diverticulum in association with ectopic ureterocele. Hinyokika Kiyo. 1988;34(8):1437–41.
- Waihenya CG. Prolapsed single system ureterocele in a female adult: case report. East Afr Med J. 2008;85(4):197–200.
- Vijay MK, Vijay P, Dutta A, Gupta A, Tiwari P, Kumar S, et al. The safety and efficacy of endoscopic incision of orthotopic ureterocele in adult. Saudi J Kidney Dis Transpl. 2011;22(6):1169–74.
- Timberlake MD, Corbett ST. Minimally invasive techniques for management of the ureterocele and ectopic ureter: upper tract versus lower tract approach. Urol Clin N Am. 2015;42(1):61–76.
- Sen I, Onaran M, Tokgoz H, Tan MO, Biri H, Bozkirli I. Prolapse of a simple ureterocele presenting as a vulval mass in a woman. Int J Urol. 2006;13(4):447–8.
- Westesson KE, Goldman HB. Prolapse of a single-system ureterocele causing urinary retention in an adult woman. Int Urogynecol J. 2013;24(10):1761–3.
Copyright @ 2016 Authors. This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original author and source are properly cited.
mji.ui.ac.id