Section Abstract Introduction Methods Results Discussion Conflict of Interest Acknowledgment References
Clinical Research
The accuracy of Aziza’s scoring system in limited slice non-enhanced thoracic CT for the diagnosis of adult pulmonary tuberculosis
pISSN: 0853-1773 • eISSN: 2252-8083
http://dx.doi.org/10.13181/mji.v26i1.1432 Med J Indones. 2017;26:40–6
Received: April 25, 2016
Accepted: February 13, 2017
Author affiliation:
1 Department of Radiology, Persahabatan Hospital, Faculty of Medicine, Universitas Indonesia, Jakarta, Indonesia
2 Department of Radiology, Faculty of Medicine, University of Gadjahmada, Yogyakarta, Indonesia
3 Department of Pulmonology, Faculty of medicine, Universitas Indonesia, Persahabatan Hospital, Jakarta, Indonesia
Corresponding author:
Aziza Icksan
E-mail: azizagicksan@yahoo.com
Background
Tuberculosis (TB) is still a major cause of morbidity and mortality in Indonesia. Thus, a fast and accurate method in diagnosing pulmonary TB (PTB) is needed, especially in adult smear-negative-TB cases. The purpose of this study was to determine the accuracy of a novel scoring system (Aziza’s score) using clinical data and characteristic abnormalities that are found in the limited slice non-enhanced thoracic CT.
Methods
This was a prospective cross-sectional study. A limited slice non-enhanced thoracic CT was performed to establish a diagnosis of PTB in patients with suspected PTB and to assess the diagnostic value of the scoring system. A reference standard used in this study was the clinical expertise of two pulmonologists. The scoring system was analyzed using bivariate and multivariate Cox regression analysis.
Results
84 of 130 suspected PTB patients were diagnosed as PTB. They were diagnosed based on pulmonary characteristic abnormalities that were found in the limited slice non-enhanced thoracic CT. The scoring system was analyzed using bivariate and multivariate Cox regression analysis. The total scores which were equal to or more than 29 could diagnose PTB with the accuracy of 96.1% (95% CIs=91.3–98.3), sensitivity of 96.5% (95% CIs=90.1–98.8), and specificity of 95.6% (95% CIs=90.1–98.8), This novel scoring method was name as an Aziza’s scoring system.
Conclusion
Aziza’s scoring system performed in the limited slice non-enhanced thoracic CT has a higher accuracy compared to the reference standard for the diagnosis of adult PTB.
Keywords
adult PTB, Aziza’s scoring system, limited slice non-enhanced thoracic CT
Pulmonary tuberculosis (PTB) is a worldwide problem. It is one of the leading causes of mortality, especially in developing countries. PTB remains as a major health problem in Indonesia.1 The gold standard for diagnosing PTB is to find Mycobacterium tuberculosis (MTB) through culture, which is difficult to perform and takes a long time.2 Nowadays, PTB is most commonly diagnosed by finding the acid-fast bacilli (AFB) in the patient’s sputum. However, in more than 50% of PTB cases, the AFB are not found in sputum examination.2 Relying upon clinical judgment in diagnosing and treating PTB will still be continued in the daily practice until an easy, fast, and cheap alternative tool is available.3,4
Currently, diagnosis of PTB is still mainly supported by a chest X-ray, especially in smearnegative TB cases. Thus, incorrect radiology expertise could mislead the management of PTB.5,6 The high resolution computed tomography (HRCT) is more sensitive (98%) compared to chest X-ray (19–58%) in showing minimal lesions, differentiating between active and non-active lesions, detecting endobronchial dissemination, and diagnosing active smear-negative PTB.2,7–15
It is important to create a standardized system using a scoring system to guide radiologists in reporting computed tomography (CT) findings when diagnosing smear-negative adult PTB. A scoring system could produce a valid and reliable evaluation of chest CT regardless of radiologists’ varying experiences and skills, and in turn, help clinicians to make an empirical judgment in treating PTB. The use of a scoring system along with limited slice non-enhanced thoracic CT is as an innovative tool in diagnostic assessment, especially in smear-negative PTB cases.
The purpose of this study was to introduce a new method in diagnosing PTB by a limited slice nonenhanced thoracic CT and report results by using this scoring system. This method could be a faster, cheaper, and more effective alternative to provide an accurate diagnosis of adult PTB compared to the reference standard.
METHODS
The protocol of this study has been approved by the ethical committee of Persahabatan Public Hospital Jakarta, Indonesia (No. 01/ KEPK-RSUP/IX/2012) and all subjects provided written informed consent. In this cross-sectional study, we consecutively collected 130 subjects from September 2012 to June 2013, who were suspected of having PTB based on the clinical symptoms and chest X-ray, but the sputum smear results were negative.
This study was conducted at the Department of Radiology, Persahabatan Hospital, Jakarta. The CT used kilovolt (KV) 120 and miliampere second (mAs) with application cared doses referenced to 100 and dose length product (DLP) ranged from 110 to 123 (Figure 1). A limited slice non-enhanced thoracic CT confined to adult TB predilection areas was performed to the suspected PTB whose sputum smear finding was negative, to reduce the radiation dose. The examined areas were the upper zone, posterosuperior apical lobes (1.2.3 right and 1/2.3 left segments) and inferior lobes (six right and left segments). To assess the spreading of lesion and pleural effusion, part of middle and the lower zone (4.5.7.8.9.10 right and left segments) were also included. The limited slice chest CT was examined by a thoracic radiologist who had 18 years of experience in the field of thoracic imaging.

Figure 1. Limited slice non-enhanced chest CT A) part of upper lung zone; B) part of middle lung zone; C) part of lower lung zone
All statistical analyses were performed using SPSS statistical software, version 20 for windows. The scoring system was calculated using bivariate and multivariate Cox regression analysis since both independent and dependent variables were dichotomous categorical data. The independent variables were age, the history of previous contact with PTB patients, the history of smoking, and nine characteristic lesions in thoracic CT: infiltrate, nodule, tree in bud opacity, consolidation, ground glass opacity, cavity, reverse halo sign, fibro calcification, and pleural effusion.
The reference standard used in this study was the expert opinions of two pulmonologists based on the subject’s clinical follow-up. The diagnosis of TB or non-TB was made two months after the antituberculosis agents (ATA) treatment based on the combination of clinical and radiological improvement, and/or positive culture result. If after two month-clinical and radiological findings showed improvement, ATA was continued even though the culture result was negative. If no improvement was shown, further diagnostic assessment had to be implemented.
RESULTS
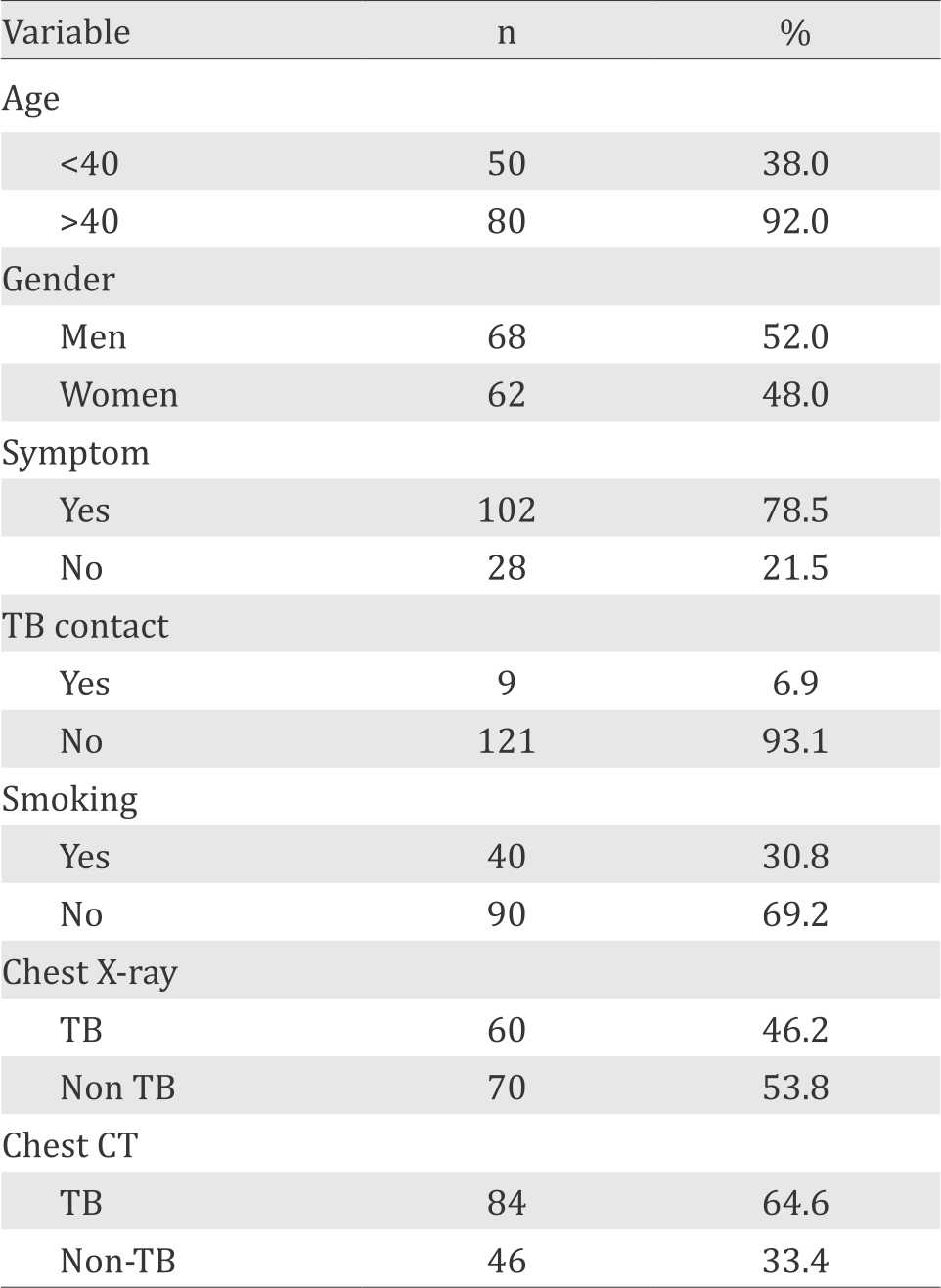
With this protocol, 84 cases of PTB were diagnosed out of 130 suspected PTB cases. The median age of subjects was 39 years old, ranging from 16 to 86 years old. The gender of the subjects was relatively equal. Only nine subjects had a history of contact with PTB patients. Forty subjects (30.7%) had history of smoking. 102 subjects had clinical symptoms, and the most common symptom was coughing more than two weeks (62.30%). Chest X-ray suggestive of PTB was found in 60 subjects, and the limited slice non-enhanced CT suspect PTB were 84 subjects. The baseline characteristics of the subjects are presented in Table 1.
Table 1. Subjects’ characteristics of suspected PTB (n=130)
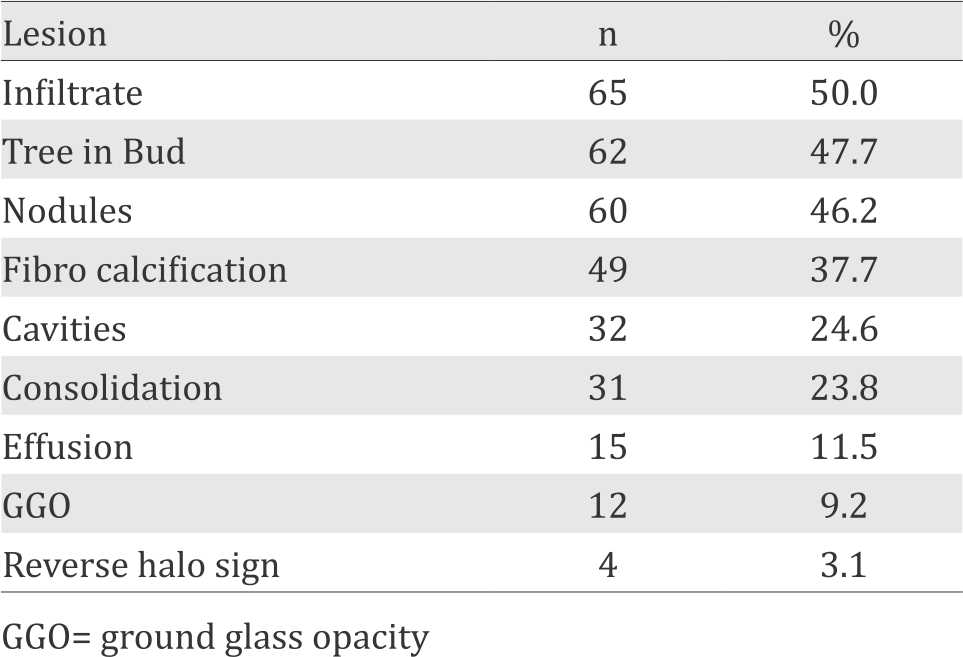
From limited slice non-enhanced thoracic CT, there were some major lesions related to PTB. The most common lesion was infiltrate (50%), followed by tree-in-bud (47.7%) and nodules (46.2%). The least common lesion was reverse halo sign, which was only found in four subjects (3.1%). The distribution of lesions is presented in Table 2.
Table 2. Main lesions PTB subjects based on limited slice non-enhanced thoracic CT (n=84)
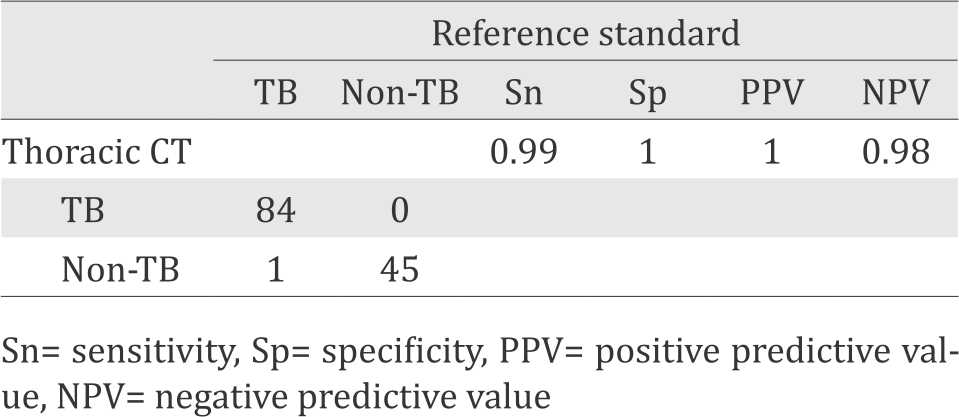
The diagnostic value of the limited slice nonenhanced thoracic CT in predicting adult PTB compared to the reference standard is presented in Table 3.
Table 3. Diagnostic value of the limited slice thoracic CT compared to the reference standard in predicting adult PTB
Scoring analysis was performed from the result of bivariate analysis between each criterion and the reference standard to see which criteria could be included in the Cox regression multivariate analysis. The results of bivariate analysis are presented in Table 4.
Table 4. Analysis between each demographic factor and several main lesions found in the limited slice thoracic CT compared with the reference standard in predicting adult pulmonary TB
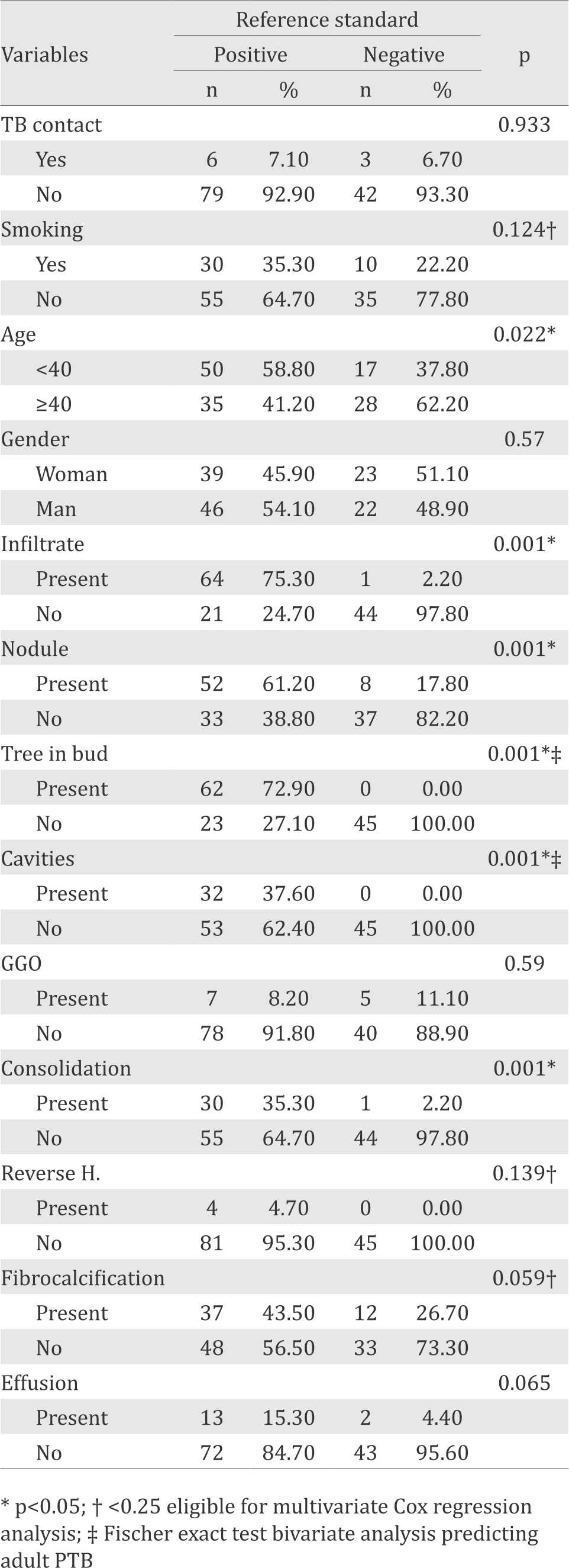
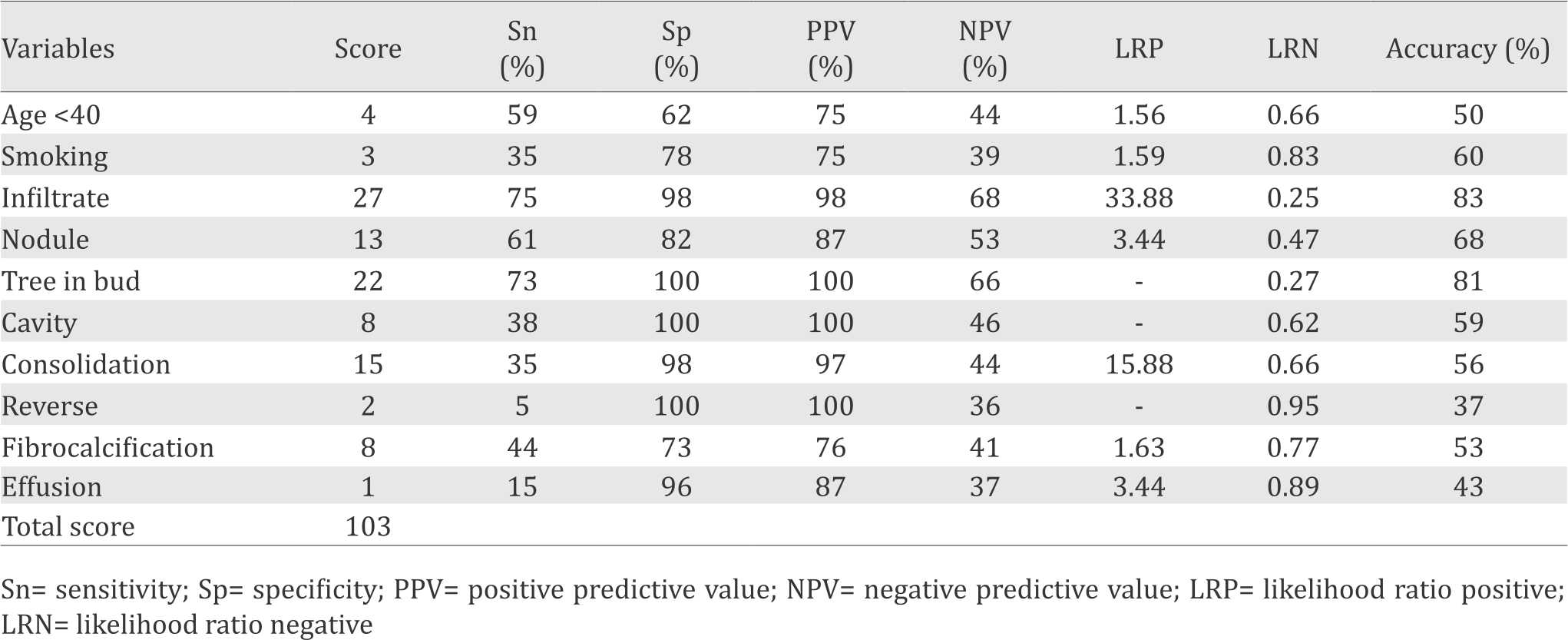
Variables included in the Cox regression multivariate analysis were the variables with p<0.25 in the bivariate analysis, i.e., eight major lesions and two demographic factors consisting of infiltrate, nodules, cavities, tree in bud, consolidation, reverse halo sign, fibro calcification, pleural effusion, age, and history of smoking. To create the scoring model, the score of each variable was calculated from the index value of Cox regression analysis by dividing every variable’s B/SE value with the lowest B/SE value, the pleural effusion’s, as a comparison. Infiltrate had the highest score value (27) with the sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of 75%, 98%, 98%, and 68%, respectively; likelihood ratio was 33.88. The result of each variable score is presented in Table 5.
Table 5. Diagnostic value of each variable score compared to the reference standard
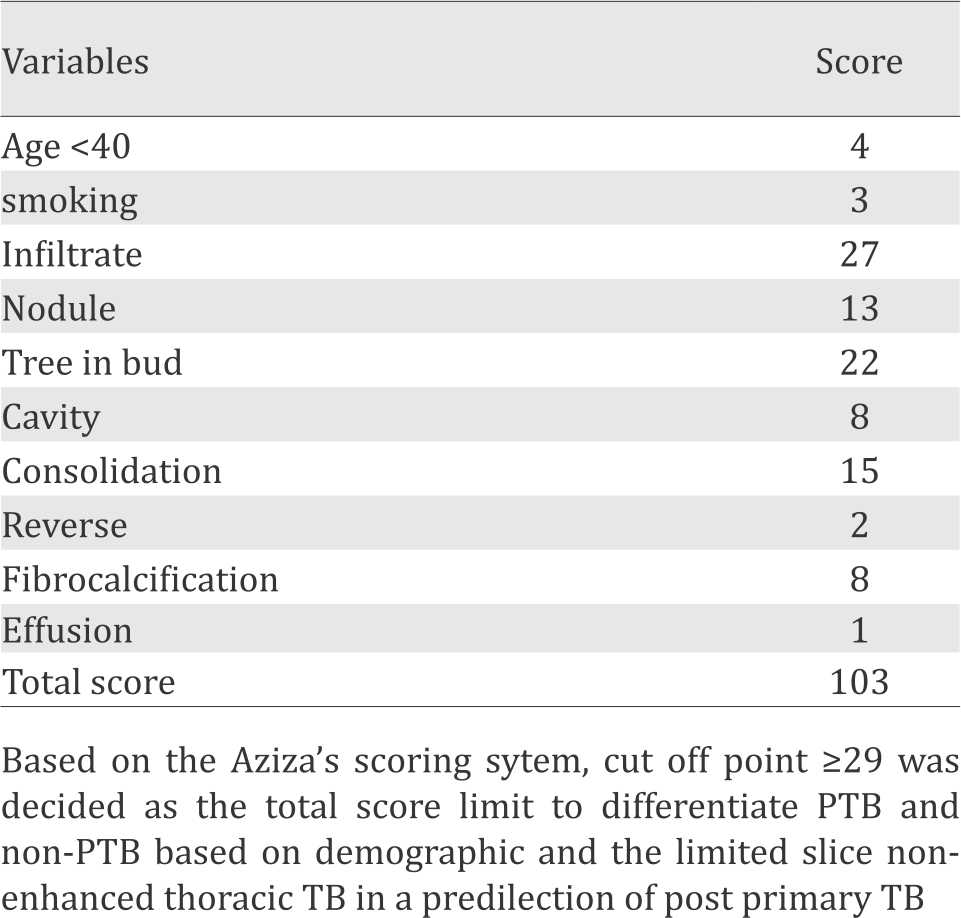
The scoring system was then applied to the subjects, and the result was compared with the reference standard in predicting PTB using receiver operating characteristic (ROC) method to acquire the cutoff point with the area under the curve (AUC) of 0.987 (0.969–1.00). A cut off point of 29 provided the most balanced sensitivity of 96.5% and specificity of 95.6% and was decided as the total score limit to differentiate PTB and non-PTB cases.
Scoring analysis
Based on the scoring system, 82 subjects had a total score of ≥29 and were diagnosed as having PTB, while from the reference standard, there were 85 subjects diagnosed as having PTB. This showed that subjects with negative findings of sputum and chest X-ray were diagnosed as negative-smear PTB after being re-examined using limited slice non-enhanced thoracic CT with Aziza’s scoring system. This result was confirmed by two experts. The summary of Aziza’s scoring system in limited slice non-enhanced thoracic CT for the diagnosis of adult PTB is presented in Table 6.
Table 6. Summary of Aziza’s scoring system in limited slice non-enhanced thoracic CT for the diagnosis of adult pulmonary tuberculosis
Among the 46 patients diagnosed as not having PTB, 18 (13.8%) patients did not have any lesion, 15 (11.5%) patients were diagnosed as having inactive TB lesion, 5 (3.8%) patients were diagnosed as having pneumonia, and 8 (6.2%) patients had other abnormalities.
DISCUSSION
This study has developed a novel scoring system in interpreting limited slice non-enhanced thoracic CT scan in a predilection area of adult PTB, aptly named Aziza’s scoring system. The scoring system could produce a valid and reliable evaluation of chest CT regardless of the radiologists’ various experiences and skills, and in turn help clinicians to make an empirical judgment in treating PTB. The proposed method is not only simple and feasible, but also has a high accuracy to distinguish between adult PTB and non-PTB, as reflected by AUC of 0.987.
The scoring system included demographic factors and main lesions in CT. The median age of the subjects was 39 years old with a range of 15 to 86 years old. Several studies have found similar results.16-19 This situation will bring socio-economic impacts for patients, families, and communities because in this age group, the level of social interaction is high. Therefore, it could increase the possibility of transmission and major problems in the future, such as permanent pulmonary disability, multidrug resistant (MDR) TB and post-PTB obstruction syndrome. Our study used the age of 40 as the cut off point, as well as one of the variables predictive of PTB based on scoring.
Forty subjects smoked, and the remaining ninety subjects did not. According to literature, smoking 15 packs/year and having long duration of smoking pose higher risk for the occurrence of PTB. Epidemiological research in South Africa reported that 50% of mortality rate is associated with smoking habit.20 Most subjects exhibited clinical symptoms, in which the most common one was coughing more than two weeks, as it was found in 81 subjects (62.3%). Similar results have been reported in several studies.17,18,21 According to literature, patients with negative smear PTB were generally asymptomatic and usually found accidentally while undergoing chest X-ray.2,8 Thus, the clinical symptoms were not included in the scoring as the current study focused on the smear-negative PTB patients.
Aziza’s scoring system is used after suspected cases are examined on limited slice nonenhanced thoracic CT scan. The statistically significant abnormalities with p=0.001 (p<0.05 from chi square test) were infiltrates (75.3%), tree in bud (72.9%), nodules (61.2%), cavity (37.6%), and consolidation (35.3%). Yadav et al2 reported slightly different findings where the major abnormalities were centrilobular nodules (91%), consolidation (38%), cavity (48%), tree in bud pattern (88%).2 Yeh et al7 performed thoracic CT in forty cases of smear-negative TB and reported findings such as centrilobular nodules (51.2%), consolidation (35%), cavity (17.5%), and tree in bud (87.5%). Tree in bud is a sign of endobronchial TB, and a sign of active PTB if it is found in areas of PTB predilection.2,7,9,12
Besides finding abnormalities associated with PTB, thoracic CT scans also find other abnormalities. This study found emphysema in 23 patients (17.7%), bronchiectasis in 16 patients (12.3%), fungal infections in three patients (2.3%) and mass in three patients (2.3%). Other studies have also found non-TB abnormalities in the thoracic CT results.9,12 This study demonstrates the superiority of thoracic CT despite performed in non-enhanced limited slices.
The limitation of this study is using clinical followup expert opinion as a reference standard. This method could be deemed as subjective, but it is the common clinical practice, even in a specialized hospital. From literature, it is said that a standard reference is the best available method to declare the patients’ disease and to ensure patients not suffering from the disease. Reference standards may be clinical follow-up, a combination of clinical follow-up and laboratory tests.22,23
In conclusion, the Aziza’s scoring system performed in limited slice non-enhanced thoracic CT has a high accuracy in diagnosing adult PTB. We propose the Aziza’s scoring system as a standard guideline in interpreting limited slice non-enhanced thoracic CT and in diagnosing adult PTB due to its benefit for smear-negative PTB cases and for early PTB case-finding.
Conflicts of Interest
The authors affirm no conflict of interest in this study.
Acknowledgment
We thank and acknowledge Aria Kekalih, MD, for his help in statistical analysis of this study.
REFERENCES
- searo.who.int [Internet]. Rencana aksi nasional programmatic management of drug resistence TB pengendalian TB Indonesia: 2011–2014 [update March 2011; cited 2012 Sept]. p. 1-5. Indonesian. Available from: http://www.searo.who.int/indonesia/topics/tb/ indonesia-ran-pmdt.pdf
- Yadav C, Gupta A, Tiwari A, Musale P. Role of imaging in management of pulmonary tuberculosis. J Evol Med Dent Sci. 2013;2(20):3457–71.
- Siddiqi K, Walley J, Khan MA, Shah K, Safdar N. Clinical guidelines to diagnose smear-negative pulmonary tuberculosis in Pakistan, a country with low-HIV prevalence. Trop Med Int Health. 2006;11(3):323–31.
- Pai M, Ramsay A, O’Brien R. Evidence-based tuberculosis diagnosis. PLoS Med. 2008;5(7):1–7.
- Icksan A, Luhur R. Radiologi toraks TB paru, 1st ed. Pradana A, ed. Jakarta: CV Sagung Seto; 2008. p. 20–44. Indonesian.
- currytbcenter.ucsf.edu [Internet]. Handbook for using the international standards for tuberculosis care (ISTC): Diagnosis and treatment public health, tuberculosis coalition for technical assistance (TBCTA) [update March 2007; cited 2012 May]. Available from: http:// www.currytbcenter.ucsf.edu/sites/default/files/istc_ handbook.pdf
- Yeh JJ, Chen SC, Teng WB, Chou CH, Hsieh SP, Lee TL, et al. Identifiying the most infectious lesions in pulmonary tuberculosis by high-resolution multi-detector computed tomography. Eur Radiol. 2010;20(9):2135–45.
- Karam MB, Masjedi MR, Fadaizadeh L, Dokouhaki P, Tahery SA, Tabatabaii SJ, et al. Role of HRCT in diagnosing active pulmonary tuberculosis. National Research Institute of tuberculosis and lung disease, Maseeh Daneshvary Hospital Teheran; Iran. 2012 [Internet]. [cited 2012 Mei 13]. Available from: http:// www.ams.ac.ir/AIM/0031/karam0031.html
- Nam KJ, Jeong YJ, Kim YD, Kim K-II, Lee JW, Park HK, et al. Chronic destructive pulmonary tuberculosis: assessment of disease activity by computed tomography. Actaradiologica. 2012;53(9):1014–9.
- Khodabakhshi, Asali A, Behnampour N, Abbasi A, Adel Barkhordar AR, Hashemi Frad A. Diagnostic value of high resolution computed tomographic scan in active pulmonary tuberculosis. J Gorgan Univ Med Sci. 2013;14(4):70–5.
- Shaarrawy H, Zeidan M, Nasr A, Nouh M. Assessment of the role of high resolution computed tomography in the diagnosis of suspected sputum smear negative active pulmonary TB. Egyptian J Chest Dis Tuberculosis. 2013;62(2):263–8.
- Feng F, Shi YX, Xia GL, Zhu Y, Lu HZ, Zhang ZY. Computed tomography in predicting smear-negative pulmonary tuberculosis in AIDS patients. Chin Med J. 2013;126(17):3228–33.
- Yoon JY, Lee IJ, Im HJ, Lee K, Lee Y, Bae SH. CT findings in apical versus basal involvement of pulmonary tuberculosis. Diagn Interv Radiol. 2013;19(2):85–90.
- Kachelriess M, Schaller S, Kalender WA. Strategies for dose reduction and improved image quality in MSCT in multi detector row CT of the thorax. 3rd ed. Berlin: Springer-verlag Heidelberg; 2004. p. 35–45.
- Kalra MK. MDCT radiation dose in MDCT a practical approach book. 1st ed. Italia: Springer verlag; 2006. p. 30–8.
- Horie T, Lien LT, Tuan LA, Tuan PL, Sakurada S, Yanai H, et al. A survey of tuberculosis prevalence in Hanoi, Vietnam. Int J Tuberc Lung Dis. 2007;11(5):562–6.
- Rasuna V. Pengamatan hasil akhir pengobatan TB paru BTA negative baru di RS Persahabatan Jakarta, Indonesia. [thesis]. Jakarta: Universitas Indonesia; 2008. p. 22-35. Indonesian.
- Icksan A, Maryastuti. Karakteristik lesi foto toraks pada TB paru BTA negatif dengan kultur negative dan kultur positif di RSUP Persahabatan Jakarta. Buletin Ilmiah Radiologi. 2014;2(1):80–9. Indonesian.
- www.who.int [Internet]. Global Tuberculosis Report USA [update June 2014; cited 2015 Sept] Available from: http://www.who.int/tb/publications/global_ report/en/
- den Boon S, van Lill SW, Borgdorff MW, Verver S, Bateman ED, Lombard CJ, et al. Association between smoking and tuberculosis infection: a population survey in a high tuberculosis incidence area. Thorax. 2005;60(7):555–7.
- den Boon S, White NW, van Lill SW, Borgdorff MW, Verver S, Lombard CJ, et al. An evaluation of symptom and chest radiographic screening in tuberculosis prevalence survey. Int J Tuberc Lung Dis. 2006;10(8):876–82.
- Whiting P, Rutjes Anne AW, Reitsma JB, Bossuyt PM, Kleijnen J. The development of QUADAS: a tool for the quality assessment of studies of diagnostic accuracy included in systematic reviews. BMC Med Res Method. 2003;3:25.
- Bossuyt PM, Reitsma JB, Bruns DE, Gatsonis CA, Glasziou PP, Irwig LM, et al. The STARD statement for reporting studies of diagnostic accuracy: explanation and elaboration. Ann Intern Med. 2003;138(1):1–23.
Copyright @ 2017 Authors. This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original author and source are properly cited.
mji.ui.ac.id