Section Abstract Introduction Methods Results Discussion Conflict Of Interest Acknowledgment References
Clinical Research
High preterm birth at Cipto Mangunkusumo Hospital as a national referral hospital in Indonesia
pISSN: 0853-1773 • eISSN: 2252-8083
http://dx.doi.org/10.13181/mji.v26i3.1454 Med J Indones. 2017;26:198–203
Received: May 26, 2016
Accepted: July 17, 2017
Author affiliation:
1 Department of Obstetrics and Gynecology, Faculty of Medicine, Universitas Indonesia, Cipto Mangunkusumo Hospital, Jakarta, Indonesia
2 Department of Obstetrics and Gynecology and Women's Health, John A Burns School of Medicine, University of Hawaii, Hawaii, U.S
Corresponding author:
Budi Iman Santoso
E-mail: budiis54@gmail.com
Background
Preterm birth is the leading direct that causes neonatal death. Indonesia was listed as one of the countries with the greatest number of preterm birth in 2010. This study aims to identify the prevalence and the potential risk factors of preterm birth among women underwent delivery in Cipto Mangunkusumo Hospital, an Indonesian national reference hospital.
Methods
This retrospective cohort study involved 2,612 women who delivered between January and December 2013. Any clinical data which related to the potential risk factors and outcomes were recorded. The data were managed using chi-square for bivariate analysis and t-test or Mann-Whitney for numerical data followed by multiple logistic regression for multivariate analysis in SPSS version 20.0.
Results
Preterm birth affected 1,020 of 2,616 pregnancies (38.5%). Non-booked patients increased nearly twice risk for preterm delivery (OR 1.89, 95% CI 1.37–2.61). While women with singleton pregnancy (OR 0.17, 95% CI 0.12–0.25), head presentation (OR 0.75, 95% CI 0.63–0.89), and regular ANC (OR 0.67, 95% CI 0.54–0.84) had lower risk for preterm birth. Apgar score, birthweight, and mode of delivery were significantly different between the pre-term group and the full-term group.
Conclusion
Prevalence of preterm birth in Cipto Mangunkusumo Hospital was approximately 2.5 times higher compared to the national number. Several factors reducing preterm birth rate include singleton pregnancy, head presentation, and regular ANC.
Keywords
outcome, preterm birth, prevalence, risk factor
Preterm birth is the leading direct cause of neonatal death.1 The rate of preterm birth has substantially increased in many locations.2 In 2010, Indonesia were listed as one of the countries with the greatest number of preterm birth. There were 15.5% preterm birth of all livebirths.3 Preterm deliveries occurred as a part of multi factorial process. Genetic, maternal, fetal and environmental factors affected the occurrence of preterm birth.4,5 Maternal age, low body mass index (BMI), multiple pregnancies were maternal factors associated with the incidence of preterm labour.5,6 Complex inflammation was the most responsible condition while infection probably has become the most clearly-understood factor.7,8
Preterm birth is associated with significant maternal, fetal, and neonatal risks. It accounts for 28% of causes in neonatal death and up to 75% of neonatal morbidity.9 In Indonesia, preterm birth contributed as many as 36% of all neonatal death causes.10 It possibly leads the newborn to neurocognitive deficits, pulmonary dysfunction and ophthalmologic disorders.9 Intrauterine fetal death (IUFD), intrauterine growth restriction (IUGR), heart rate abnormalities, early onset neonatal sepsis, intraventricular hemorrhage, cerebral palsy, anemia, constipation, and twintwin transfusion syndrome were also associated with the preterm deliveries.7,11 These situations raise the needs for local epidemiological study of preterm birth in every level hospital in Indonesia. One of the tertiary national referral center hospital in Indonesia is Dr. Cipto Mangunkusumo Hospital. We assume that the prevalence of preterm birth in tertiary referral hospital will be higher than other hospitals because preterm delivery, especially the babies, needs advanced technology to increase the neonatal survival rate. Therefore, this study aims to determine the prevalence and potential risk factors for preterm birth among women underwent delivery in Dr. Cipto Mangunkusumo Hospital. The authors hope that by determining this prevalence and risk factors, the clinician, especially obstetrician, can perform strategic step to protect and early diagnose of preterm birth.
METHODS
The database used in this study was collected from the medical record of patients during the year of 2013. For each patient, we entered demographics, obstetric history, diagnosis, management, laboratory data, as well as maternal and neonatal outcomes. Maternal age was classified into less than 20, 20 to 35 and more than 35 years old because the optimal and recommended reproductive age is 20 to 35 years old. Validated clinical information was recorded into the database in a consistent manner. Noncomplete medical records were included in this study. However, for each analysis, medical records without required data have been excluded. The data for all patients were entered by a single data manager at the end of study period. The study has been approved by the Institutional Review Board at University of Indonesia number 503/H2.F1/ ETIK/2014.
Retrospective analysis was conducted on the entire cohort of singleton and twin pregnancies. The patient could be both of booked and non-booked cases. The primary independent variable for this study was maternal age, number of fetus (single or multiple), parity, previous cesarean section (CS), referral type (booked-case or not), regularity of antenatal care (ANC), and leukocytes count at presentation. Gestational age was analyzed categorically as fullterm (≥37 weeks), extremely preterm (<28 weeks), very preterm (28–<32 weeks), and moderate or late preterm (32–<37 weeks) newborns. Several preterm birth outcomes such as methods of delivery, Apgar score, birth weight, and amniotic fluid color (color of amniotic fluid observed during labor) were studied secondarily.
IBM SPSS Statistics version 20.0 was used for statistical analyses. Bivariate analyses for categorical data using chi-square was performed to findthe association between preterm birth and independent t-test or Mann-Whitney test used for numerical data. We considered p value <0.05 as statistically significant. Multiple logistic regression analysis with a backward elimination stepwise regression approach was used to evaluate the association between preterm delivery and potential risk factors. Adjusted odds ratios with their confidence intervals were used to describe the relative risk of the potential risk factors.
RESULTS
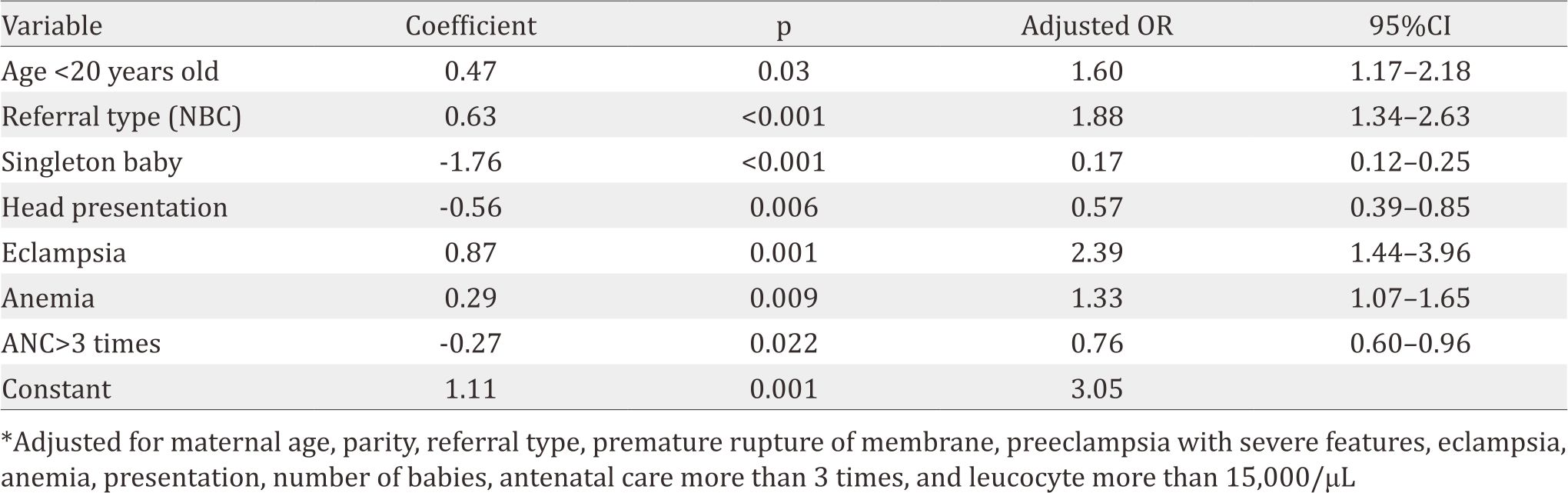
Preterm birth affected 1,020 of 2,616 (38.5%) all pregnancies was analyzed. Moderate to late preterm births were accounted for 67.4% of all preterm births while very preterm and extremely preterm were 22.9% and 9.7%, respectively. The preterm birth cohort was characterized by a significantly higher prevalence of women aged 20–33, multiparous, non-booked cases patients, and singleton head presentation. Incomplete fields were not eligible for analysis. Therefore, the number of subjects for each bivariate analysis resulted in various number (Table 1). Maternal age, referral type, presentation, number of babies, and regularity of ANC were associated with preterm birth (Table 2). In multivariate analysis, age less than 20 years old, referral type, eclampsia, and anemia increased the risk of preterm birth while singleton baby, head presentation, and regular ANC reduced the risk (Table 3).
Table 1. Distribution of gestational age at birth according to gestational age group and subgroup
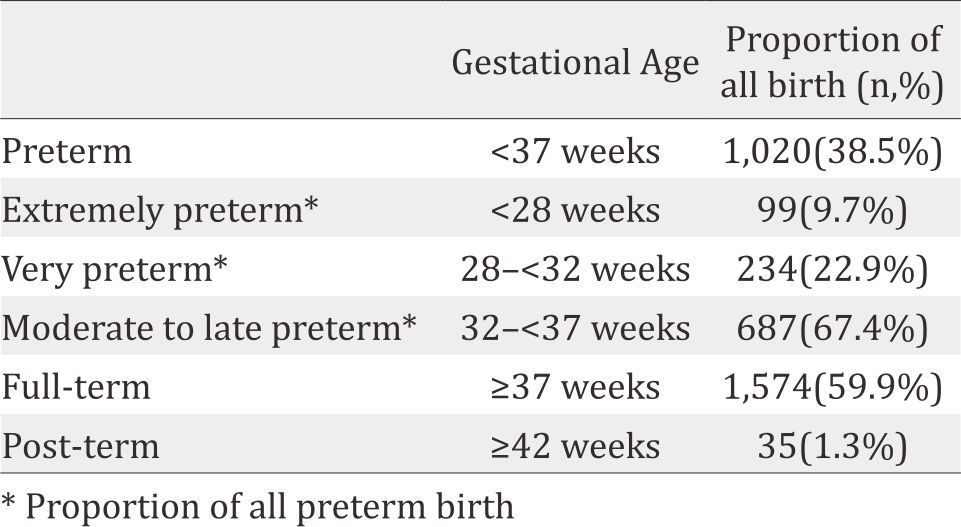
Table 2. Clinical characteristics of pregnancies according to gestational age at deliveries
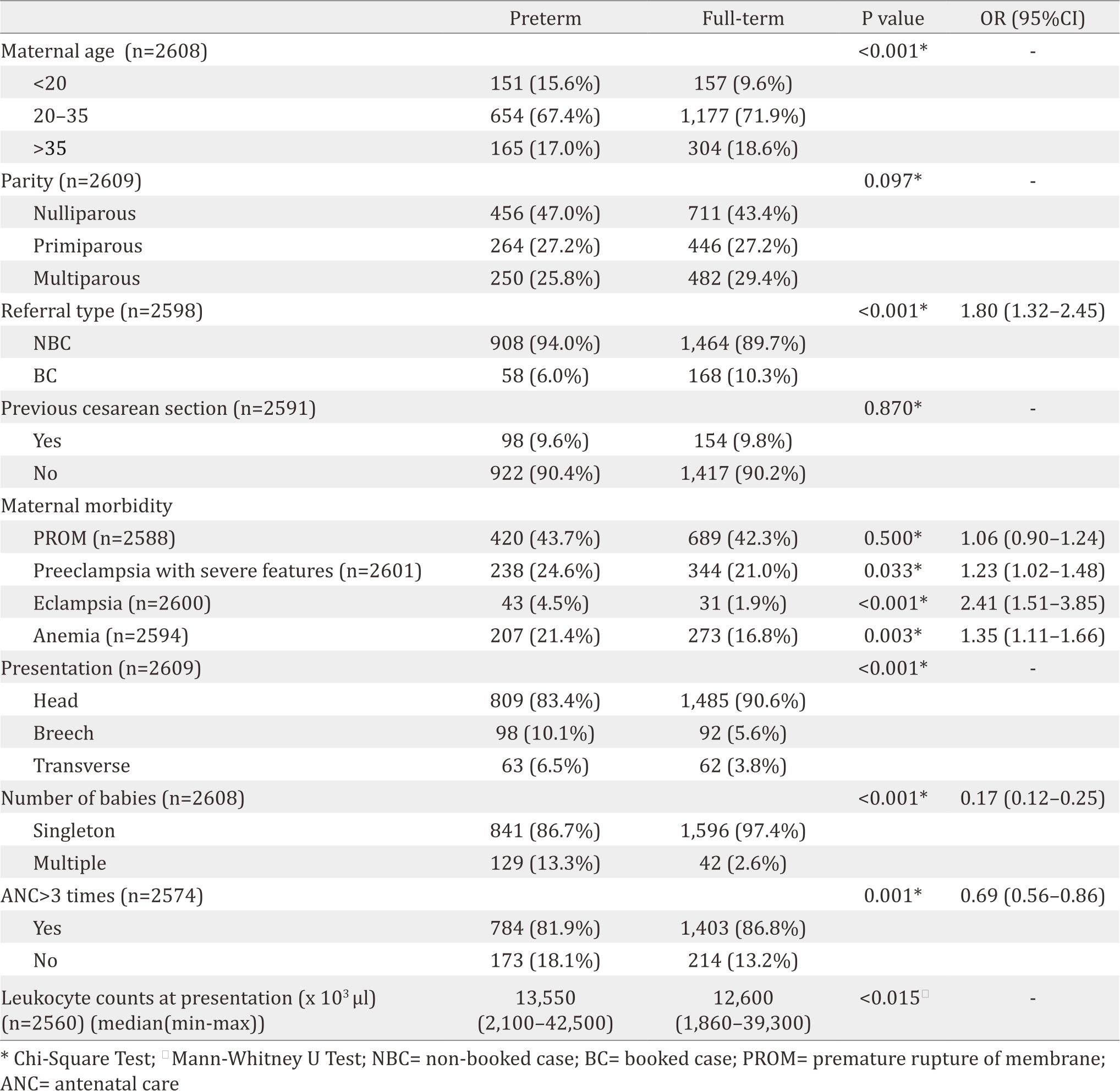
Table 3. Results of multiple logistic regression analysis on risk and protective factors for preterm delivery*
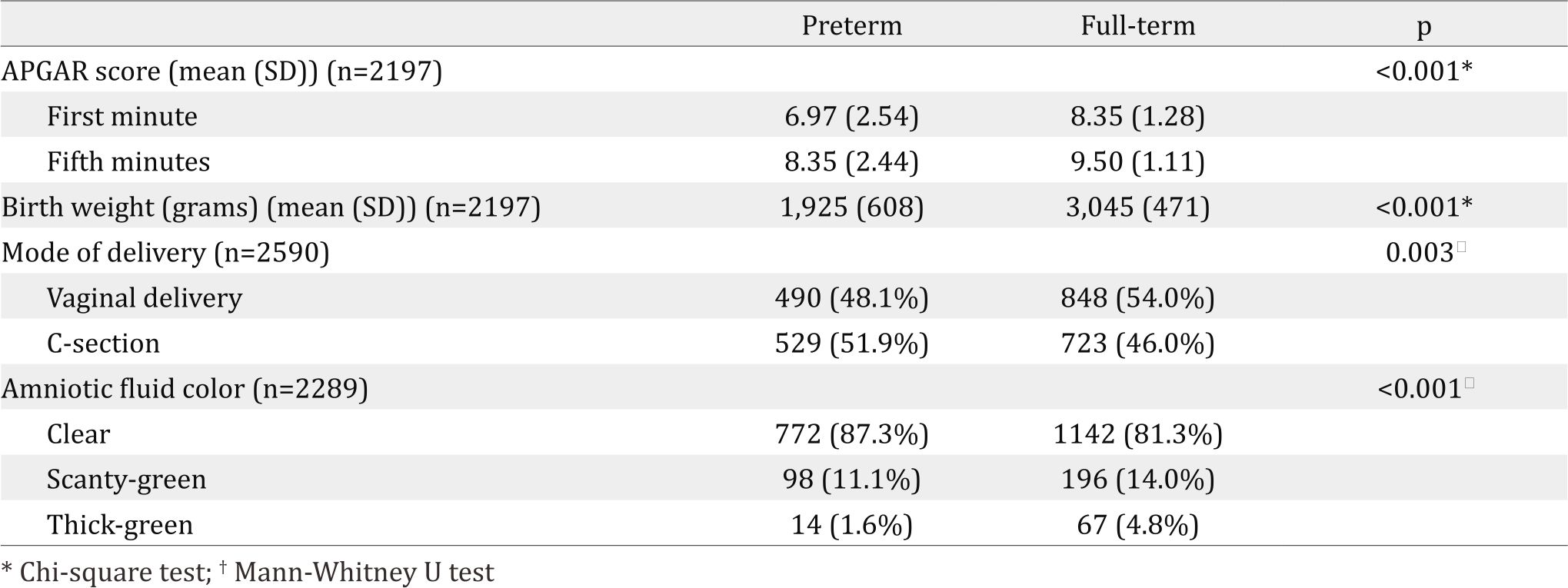
Apgar score, birthweight, need for induction, and mode of delivery were significantly different between the pre-term group and the full-term group (Table 4). Apgar score and birthweight were significantly lower in the preterm group. Preterm pregnancy significantly led to higher cesarean section rate compared to the full-term group.
Table 4. Perinatal outcomes associated with preterm birth according to gestational age at deliveries
DISCUSSION
To best knowledge, this is the largest hospitalbased study finding at preterm birth prevalence in Indonesia. The prevalence of preterm birth in this study was 2.5 times higher compared to the national prevalence (15.5%). It is predominantly affected by the high number of referral cases to this hospital. In accordance with a systematic review on prevalence of preterm birth, moderate to late preterm birth rate was the highest proportion of all preterm deliveries.3 The result was similar with our study (67.4% cases of moderate to late preterm birth). Application of standard preterm definitions is important to study the survival probability of the neonates.3
Primiparity did not increase the risk for preterm birth in our study. However, Erez et al12 concluded that primiparity was the independent risk factors for preterm delivery (OR 1.45, 95% CI 1.18- 1.78). The age distribution of our population was similar to a study conducted by Chen et al. among upper middle class in Chinese population.13 The percentage of women aged below 20 years old were higher in the preterm group compared to the non-preterm group in our study. Moreover, the association between maternal age and preterm birth was statistically significant. Nguyen et al14 found that women aged 24 or below were tend to deliver preterm babies 1.9 times compared to 24–35 years old women. Meanwhile, a systematic review found that older maternal age was associated with preterm birth.15 Therefore, there is insufficient evidence to conclude that older or younger maternal age is an independent risk factor for preterm birth.
This study did not find correlation between previous CS with preterm birth. Conversely, Di Renzo et al. found approximately three times increased risk for spontaneous preterm birth in women underwent previous CS.16 Regular ANC was one of the independent protective factors for having preterm birth. It had been described previously by Bastek,17 which stated that no prenatal care was one of the components in prediction models of women for having delivery before 37 weeks.
Singleton pregnancy revealed a reduced risk to preterm labor (p<0.001; OR 0.17; 95% CI 0.12- 0.25). Nice Clinical Guidelines stated that more than 50% of twins and almost all triplets were born before 37 weeks of gestation, and 15–20% would be admitted in neonatal unit related to preterm.18 In this study, there was a significant association between white blood cell count and prevalence of preterm birth. However, it did not affect in multivariate analysis. Surabhi et al19 stated that stress of delivery may lead to brisk leukocytosis. Apart from that, the increase of white blood cell was usually identified in patients with intrauterine infection and adverse perinatal outcome. Nevertheless, amniotic fluid white blood cell was a better independent predictor than white blood cell.
Significant lower birthweight was found in most of preterm studies.20,21 The birthweight of preterm babies in this study was 1,925 grams. It is comparable with 33–35 weeks gestation babies delivered in ten California and Massachusetts hospitals, ranging from 1,759 to 2,215 grams.22 In another large study, the birthweight of 34– 36 weeks babies ranged from 2,195 to 2,687 grams.21 Very preterm babies included in the analysis could lower the mean of birthweight. Apgar scores in both 1st and 5th minutes were significantly associated with preterm birth. It had been previously described in China, with Apgar score on 1st min and 5th min was 7.7 (SD 2.43) and 8.9 (SD 1.81).13 Consequently, this situation will possibly lead to the substantial risk for neonatal deaths.20
The limitation of this study is that we collected the data from a tertiary, national referral hospital. Thus, the result might be hardly applied in general setting. The Apgar score was prepared by the attending neonatologist or neonatology residents. This could possibly lead to bias secondary to inter-practitioner variability in diagnostic criteria. However, it is difficult to eliminate this potential bias due to the academic hospital system.
In conclusion, prevalence of preterm birth in Dr. Cipto Mangunkusumo Hospital was approximately 2.5 times higher compared to national number. Several factors reducing the preterm birth rate include singleton pregnancy, head presentation, and regular ANC.
Conflicts of Interest
The authors affirm no conflict of interest in this study.
Acknowledgment
Thank to all midwives, nurses, obstetrics and gynecology residents for their help in collecting data for preparing the manuscript.
REFERENCES
- Lawn JE, Gravett MG, Nunes TM, Rubens CE, Stanton C, GAPPS Review Group. Global report on preterm birth and stillbirth (1 of 7): definitions, description of the burden and opportunities to improve data. BMC Pregnancy Childbirth. 2010;10 Suppl 1:S1.
- Goldenberg RL, Culhane JF, Iams JD, Romero R. Epidemiology and causes of preterm birth. Lancet. 2008;371(9606):75–84.
- Blencowe H, Cousens S, Oestergaard MZ, Chou D, Moller A-B, Narwal R, et al. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: a systematic analysis and implications. Lancet. 2012;379(9832):2162–72.
- Warren JE, Silver RM. Genetics of the Cervix in Relation to Preterm Birth. Semin Perinatol. 2009;33(5):308–11.
- Murphy DJ. Epidemiology and environmental factors in preterm labour. Best Pract Res Clin Obstet Gynaecol. 2007;21(5):773–89.
- Lo CC, Hsu JJ, Hsieh CC, Hsieh TT, Hung T-H. Risk Factors for Spontaneous Preterm Delivery Before 34 Weeks of Gestation Among Taiwanese Women. Taiwan J Obstet Gynecol. 2007;46(4):389–94.
- Hofer N, Kothari R, Morris N, Müller W, Resch B. The fetal inflammatory response syndrome is a risk factor for morbidity in preterm neonates. Am J Obstet Gynecol. 2013 Dec;209(6):542.e1–542.e11.
- Olgun NS, Reznik SE. The matrix metalloproteases and endothelin-1 in infection-associated preterm birth. Obstet Gynecol Int. 2010;2010(11):1–8.
- Wen SW, Smith G, Yang Q, Walker M. Epidemiology of preterm birth and neonatal outcome. Semin Fetal Neonatal Med. 2004;9(6):429–35.
- UNICEF [Internet]. Maternal, Newborn & Child Survival. [update 2008 ; cited 2017]. Availabe from : www.unicef. org/eapro/Indonesia_Eng.pdf. p. 1–4.
- Zachariassen G, Fenger-Gron J. Preterm dietary study: meal frequency, regurgitation and the surprisingly high use of laxatives among formula-fed infants following discharge. Acta Paediatr. 2014 Mar;103(3):e116–22.
- Erez O, Mayer A, Shoham-Vardi I, Dukler D, Mazor M. Primiparity, assisted reproduction, and preterm birth in twin pregnancies: a population based study. Arch Gynecol Obstet. 2007 Oct 31;277(4):311–7.
- Chen CP, Wang KG, Yang YC, See LC. Risk factors for preterm birth in an upper middle class Chinese population. Eur J Obstet Gynecol. 1996 Dec;70(1):53–9.
- Nguyen N, Savitz DA, Thorp JM. Risk factors for preterm birth in Vietnam. Int J Gynecol Obstet. 2004;86(1):70–8.
- Newburn-Cook CV, Onyskiw JE. Is older maternal age a risk factor for preterm birth and fetal growth restriction? A systematic review. Health Care Women Int. 2005;26(9):852–75.
- Di Renzo GC, Giardina I, Rosati A, Clerici G, Torricelli M, Petraglia F, et al. Maternal risk factors for preterm birth: a country-based population analysis. Eur J Obstet Gynecol Reprod Biol. 2011 Dec;159(2):342–6.
- Bastek JA, Sammel MD, Srinivas SK, McShea MA, Foreman MN, Elovitz MA, et al. Clinical prediction rules for preterm birth in patients presenting with preterm labor. Obstet Gynecol. 2012;119(6):1119–28.
- Nice Clinical Guidelines. Multiple pregnancy: The management of twin and triplet pregnancies in the antenatal period. RCOG; 2011.
- Chandra S, Tripathi AK, Mishra S, Amzarul M, Vaish AK. Physiological changes in hematological parameters during pregnancy. Indian J Hematol Blood Transfus. 2012; 28(3):144–6.
- Marchant T, Willey B, Katz J, Clarke S, Kariuki S, Kuile FT, et al. Neonatal Mortality Risk Associated with Preterm Birth in East Africa, Adjusted by Weight for Gestational Age: Individual Participant Level Meta-Analysis. PLoS Med. 2012;9(8):e1001292.
- Gouyon JB, Vintejoux A, Sagot P, Burguet A, Quantin C, Ferdynus C, et al. Neonatal outcome associated with singleton birth at 34–41 weeks of gestation. Int J Epidemiol. 2010;39(3):769–76.
- McCormick MC, Escobar GJ, Zheng Z, Richardson DK. Place of birth and variations in management of late preterm (“near-term”) infants. Semin Perinatol. 2006;30(1):44–7.
Copyright @ 2017 Authors. This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original author and source are properly cited.
mji.ui.ac.id