Section Abstract Introduction Methods Results Discussion Conflict of Interest Acknowledgment References
Clinical Research
Cardiovascular response and backward, upward, right push maneuver during laryngoscopy: comparison between CMAC® video laryngoscopy and conventional Macintosh
pISSN: 0853-1773 • eISSN: 2252-8083
https://doi.org/10.13181/mji.v26i2.1505 Med J Indones. 2017;26:116–21
Received: July 20, 2016
Accepted: May 21, 2017
Author affiliation:
Department of Anesthesiology and Intensive Therapy, Faculty of Medicine, Cipto Mangunkusumo Hospital, Universitas Indonesia, Jakarta, Indonesia
Corresponding author:
Arif H.M. Marsaban
E-mail: arifhmm@yahoo.co.id
Background
Increased blood pressure and heart rate are the most frequent response to laryngoscopy which sometimes causes serious complications. Laryngoscopy technique and tools modification lessen the nociceptive stimulation, thus preventing hemodynamic response. BURP maneuver is used to lower Cormack-Lehane level, but it can cause additional pain stimulation during laryngoscopy. The aim of this study was to compare the cardiovascular response and the need of BURP maneuver during laryngoscopy between CMAC® and conventional Macintosh.
Methods
A randomized, single blinded, control trial was performed to 139 subjects who underwent general anesthesia with endotracheal tube. Subjects were randomised into a control group (conventional Macintosh) and an intervention group (CMAC®). The cardiovascular parameters (systolic, dyastolic, mean arterial pressure, and heart rate) were measured prior to induction (T1). Midazolam 0.05 mg/kg and Fentanyl 2 micrograms/kg were given 2 minutes before the induction. Moreover, they were given propofol 1 mg/kg followed by propofol infusion of 10 mg/kg/hour and Atracurium 0.8–1 mg/kg. After TOF-0 cardiovascular parameters (T2) were remeasured, it was proceeded to laryngoscopy. When Cormack-Lehane 1–2 was reached (with or without BURP maneuver), cardiovascular parameters were measured again (T3).
Results
Unpaired T-test showed that cardiovascular response during laryngoscopy were significantly lower in the intervention group compared to the control group (p<0.05). The need of BURP maneuver was significantly lower in the CMAC® group compared to the Convensional Macintosh group (13.9% vs 40.3%; p<0.05).
Conclusion
Cardiovascular response and BURP maneuver during laryngoscopy with CMAC® were significantly lower compared to conventional Macintosh.
Keywords
BURP maneuver, cardiovascular response, CMAC®, conventional Macintosh, laringoscopy
Laryngoscopy creates painful stimuli, resulting in cardiovascular response in the form of increased blood pressure and heart rate. Although these responses are transient, they could be problematic for patients with cardiac diseases and intracranial lesion.1 Higher dose intravenous opioid and intravenous lidocaine cannot repress cardiovascular response totally.2 Inhalation agents used to deepen anesthesia cause blood pressure drop, resulting in poor coronary and brain perfusion. Neural blockage in airway needs special skills and experiences due to the difficulty level and high risk of local anesthesia injection into the vessels. Topical anesthesia use in the airway is still in research.3 Cardiovascular blocker drugs such as bisoprolol or esmolol can be given, but sympathetic activity would be repressed leading to decreased coronary perfusion.4 Laryngoscopy technique and tools modification lessen the nociceptive stimulation, thus preventing hemodynamic response.5,6
Backward, upward, right push (BURP) maneuver is a maneuver to push larynx from outside, to get a better larynx visualization during laryngoscopy. Laryngoscopy will push larynx downward (caudal), upward (anterior) and to the left. BURP maneuver positioned larynx to its original position, and the epiglottis is still lifted, creating an optimal visualization of larynx and glottis.7–9
Laryngoscopy video’s role is increasing in the last 10 years, especially for difficult airway management. The larynx was visualized better, decreasing failed intubation.10–12 The advantages of CMAC® such as increased successful first attempt of intubation, shorter laryngoscopy duration, and decreasing Cormack-Lehane grade interest the researchers to compare the cardiovascular responses and BURP maneuver necessity during laryngoscopy between video laryngoscopy CMAC® and the conventional Macintosh.
METHODS
After getting approval from the ethics committee, the Faculty of Medicine Universitas Indonesia, Cipto Mangunkusumo Hospital and consents from patients (No. 878/UN2.F1/ETIK/2015), a randomised, single blinded, control trial was conducted in Cipto Mangunkusumo Hospital, Jakarta from October to December 2015. Population was surgery patients who underwent general anesthesia with endotracheal intubation in Cipto Mangunkusumo Hospital.
The inclusion criteria were adult (18–65) years old, body mass index (BMI) 18.5–30 kg/m2, physical status American Society of Anesthesiology (ASA) 1–2, and have consented to participate in this study. The exclusion criteria were pregnancy, history of cardiac diseases, cerebrovascular disease history, hypertension, hypotension, tachycardia, bradycardia, patients consuming cardiovascular drugs, difficult airway suspicion, increased intracranial pressure, and converted general anesthesia patients from regional anesthesia. Furthermore, the dropout criteria were patients who moved during laryngoscopy, patients with desaturation or other emergencies, train-of-four (TOF) score did not reach 0 with induction and relaxation dose according to study protocol, Cormack-Lehane level other than 1 or 2 at the first laryngoscopy attempt with BURP maneuver (60 seconds maximum).
Samples were obtained through non probability sampling with consecutive sampling. Randomization for subjects was done with block randomization using tables. The sample size was calculated using analytic categorical sample size formula for unpaired two groups. Proportion was obtained from previous research. The subjects were divided into two groups of laryngoscopy; the Macintosh blade group and the video laryngoscopy CMAC® group.
The recorded data were name, age, sex, medical record, height, weight, and ASA status. A vital signs monitor was put on patients on the operating table. Systolic and diastolic blood pressure, mean arterial pressure, and heart rate were recorded/ time-1 (T1). Both groups received midazolam 0.05 mg/kgBW and fentanyl 2 mcg/kgBW intravenous, oxygen 80 via face mask, tidal volume 6–8 mL/kgBW, and respiratory rate 12–14 x/minute. Two minutes after midazolam and fentanyl administration, induction with propofol 10 mg/kgBW was done, followed by continued infusion of propofol 10mg/kg/hour. Atracurium 0.8–1 mg/kgBW was given after eyelashes reflect was lost. After TOF score was 0, systolic and diastolic blood pressure, mean arterial pressure, and heart rate were recorded/ time-2 (T2). Laryngoscopy was performed until Cormack-Lehane grade 1 or 2 for larynx visualization achieved, maximum 60 minutes according to the designated laryngoscopy group. Systolic and diastolic blood pressure, mean arterial pressure, heart rate and BURP maneuver were recorded/ time-3 (T3).
Patients were given face mask, excluded, and treated with the ASA algorithm if laryngeal visualization was failed. In cases of emergency, the advance life support (ALS) and basic life support (BLS) algorithms were done, and patients were excluded.
T1-T2 was analyzed with unpaired T-test, and the result was p>0.05 (not significant difference) in every cardiovascular parameter. This result showed that two groups met the same effect of induction, and there was no confounding factor between two groups.
Data were analysed using statistical product and service solutions (SPSS) Cardiovascular response and unpaired T-test and Mann-Whitney-U test as alternative test methods. BURP maneuver was analyzed with a Chi-squared and a fisher test as alternative test methods.
RESULTS
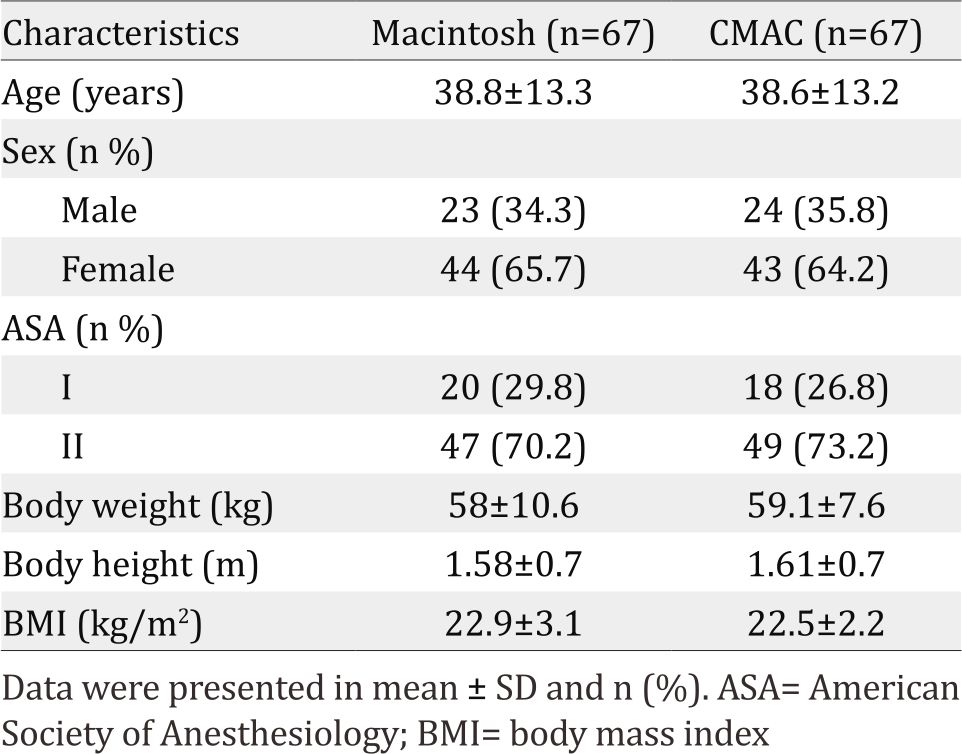
The research flowchart was presented in Figure 1. Table 1 shows subjects’ characteristic.
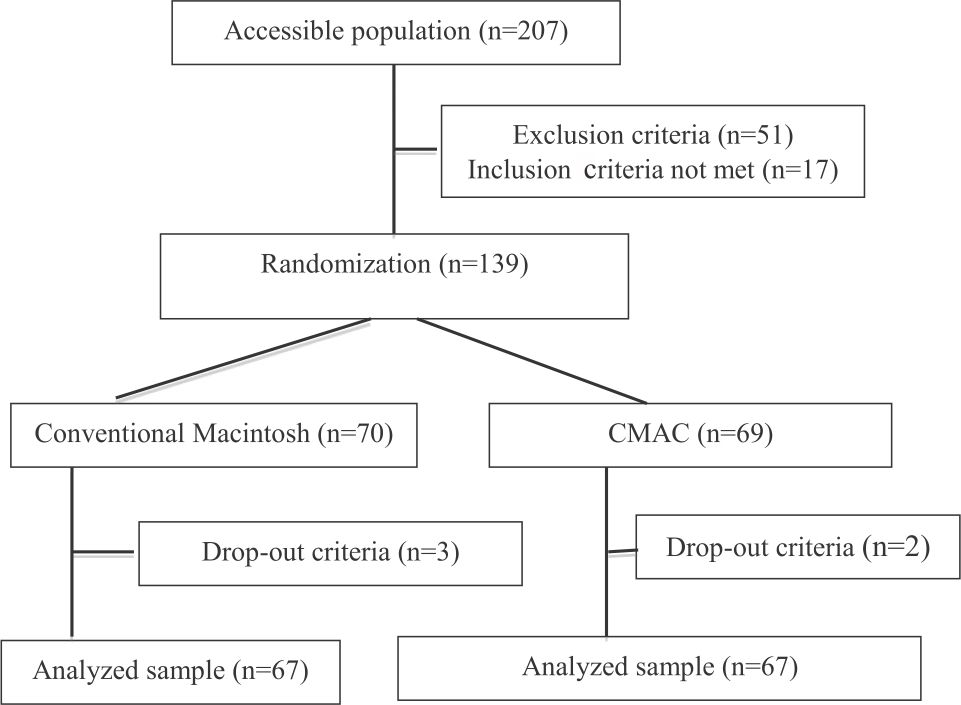
Figure 1. Consolidated standards of reporting trials (CONSORT) flow-chart
Table 1. Subjects’ characteristics
Cardiovascular responses were shown in Figure 2. It showed the difference between T1-T2 and T2- T3. T1-T2 difference showed a decreasing trend, which means the cardiovascular parameters declined after induction. T2-T3 difference showed an increasing trend.
Figure 3 showed statistical tests done to investigate differences in the variables between Macintosh intubation and CMAC® intubation. Systolic blood pressure (CI 95%=5.58-14.44), diastolic blood pressure (CI 95%=2.93-9.54), and heart rate (CI 95%=2.26-8.66) showed a significant T2-T3 difference.
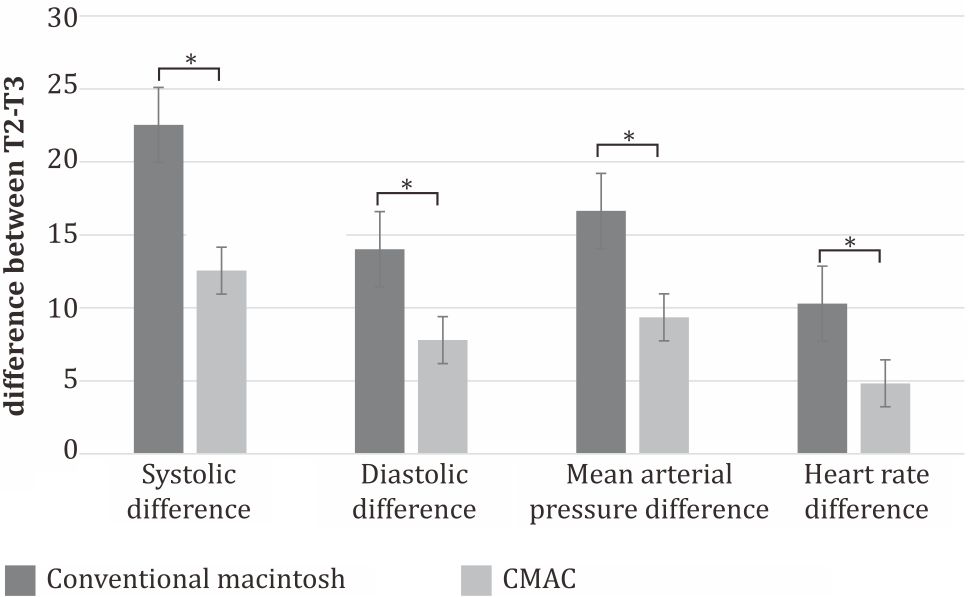
Figure 3. Statistical test for cardiovascular parameter difference between T2-T3 represented cardiovascular response due to laryngoscopy. T1-T2 (not shown) was analyzed with unpaired t-test, and the result was p>0.05 (not significant difference) in every cardiovascular parameter. This result showed that two groups met the same effect of induction, and there was no confounding factor between two groups. *p<0.001
Table 2 showed BURP maneuver necessity between Macintosh and CMAC®. Figure 4 showed illustration between conventional Macintosh and CMAC equipment and the effects in larynx.
Table 2. BURP naneuver necessity
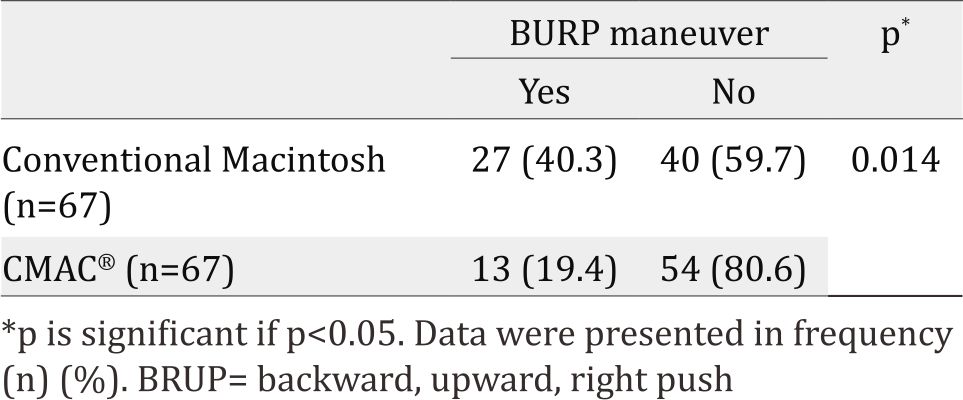
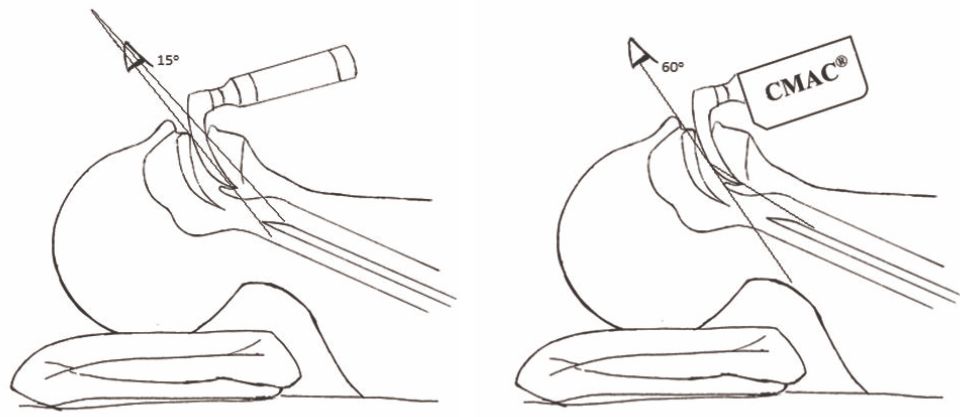
Figure 4. Illustration between conventional Macintosh and CMAC® equipment and the effect in larynx
DISCUSSION
This study evaluated cardiovascular parameters such as systolic and diastolic blood pressure, mean arterial pressure, heart rate, and BURP maneuver necessity during laryngoscopy to achieve Cormack-Lehane grade 1 or 2. Cardiovascular parameter of T1 of each group were not different (Table 1), means confounding factors of cardiovascular parameters before induction and during induction were eliminated through inclusion and exclusion criteria. Biometric factors (age, height, weight, BMI) could affect the airway anatomy and airway management difficulty; thus, the inclusion criteria included age and BMI. ASA physical status was limited to 1 and 2 in order for methods to be applied to all subjects and to lessen preoperative confounding factors (e.g. hypovolemia, cardiovascular drugs, arrhythmia, etc.).
Both groups were given similar drug types and doses to eliminate confounding factors. To avoid hypercarbia as a confounding factor of cardiovascular response, laryngoscopy duration was limited to 60 seconds.13
The Macintosh group showed a significant larger change of the parameters in T2-T3 compared to the CMAC® group. This change was induced by pain during the procedure. Laryngoscopy using Macintosh blade required a laryngeal lift maneuver, so the larynx axis was in line with the operator’s eye axis.8,14 Mechanical pain stimulation due to the blade was sensed by the nociceptors in the tongue base mucosa, valecula, and anterior epiglottis surface. Neural stimulus traveled to suprarenal gland, inducing catecholamine release, and thus, it increased sympathic activities such as blood pressure and heart rate.15,16 The difference between Macintosh and CMAC® showed different pain stimuli produced by each method. CMAC® has a camera at the end of its blade. The camera would be in front of the larynx in laryngoscopy. Cormack-Lehane grade 1 or 2 can be achieved by slightly lifting larynx up, which is in accordance with Noppens’ study17 that stated CMAC® showed better laryngeal visualization; therefore, pain stimulus and catecholamine release were decreased.17 CMAC® has wider visualization than Macintosh (60° vs 15°),18 aid to achieve better visualization of larynx and minimize pain stimulus, time for intubation, and BURP maneuver needs.19
Heart rate showed the smallest change compared to other parameters. T3 heart rate in Macintosh was 10.29±10.41 bpm and in CMAC® was 10.29±10.41 bpm. This might be the result of fentanyl administration 5–6 minutes before laryngoscopy. After 5–6 minutes, fentanyl reached its peak plasma concentration. Fentanyl 2 mcg/ kgBW and propofol induction can decreased sinoatrial node frequency.20 Study showed that heart rate during induction was 11–27% lower than pre-induction state, while it decreased 7–15% as laryngoscopy response.
BURP maneuver was less needed in the CMAC® group compared to the Macintosh group since the camera in CMAC® blade was almost directly in front of the larynx, facilitating Cormack- Lehane I or II visualization.17,21 Facilitation from CMAC® video laryngoscopy in larynx visualization had lesser painful stimulus during laryngoscopy procedure compared with the Macintosh visualization, which resulted in lower cardiovascular responses in the CMAC® group compared to the Macintosh group significantly. BURP maneuver, in other hand, could create additional painful stimulus. BURP maneuver exerted pressure to larynx from the outside at the same time when the blade pressed tonguebase, valecula, and anterior epiglottis surface, resulting in simultaneous painful stimuli.
Blood pressure and mean arterial pressure were measured by a non-invasive blood pressure monitor, requiring 20–40 seconds to measure. This method is a standard observation procedure from ASA. Intra-arterial observation is more invasive and more expensive. Confounding factors of cardiovascular parameters were posed by BURP maneuver’s association with the parameters and required time to achieve Cormack-Lehan 1 or 2 (from the start of laryngoscopy). Since these are not the aim of the studies, data regarding these were not analyzed.
We suggest further studies measuring blood catecholamine level during laryngoscopy and BURP maneuver in association with cardiovascular parameters needs to be done. Blood catecholamine level increases with pain stimuli, in order that, we can compare the response of pain stimuli better due to Macintosh and CMAC®. Limitation of this study included catecholamine level that was not measured as a response to laryngoscopy due to high cost of this laboratory examination. Cardiovascular changes were assumed due to painful stimuli of laryngoscopy.
In conclusion, cardiovascular response and BURP maneuver during laryngoscopy with CMAC® video laryngoscopy were significantly lower compared to conventional Macintosh.
Conflicts of Interest
The authors affirm no conflict of interest in this study.
Acknowledgment
There is no conflict of interest including any financial interests or financial conflicts to declare relating to the past 5 years or the foreseeable future. The study was supported by Department of Anesthesiology and Intensive Care, Faculty of Medicine, Universitas Indonesia.
REFERENCES
- Hagberg CA, Artime CA. Airway management in adult. In: Miller RD, Weiner-Kronish JP, Young WL, editors. Miller’s anesthesia. 8th ed. Philadelphia. Elsevier Saunders; 2015. p. 1647–83.
- Hassani V, Movassaghi G, Goodarzi V, Safari S. Comparison of fentanyl and fentanyl plus lidocaine on attenuation of hemodynamic responses to tracheal intubation in controlled hypertensive patients undergoing general anesthesia. Anesth Pain Med. 2013;2(3):115–8.
- Chaundary B, Shah SM, Sarvaiya VU. Comparative study of two different doses of fentanyl citrate 2 microgram/ kg and 4 microgram/kg intravenous in attenuation of hemodynamic responses during intubation. NHL Journal of Medical Science. 2013;2(2):41–3.
- Deem SA, Bishop MJ, Bedford RF. Physiologic and patophysiologic responses to intubation. In: Hagberg CA, editor. Benumof’s airway management. 2nd ed. Philadelphia. Mosby Inc; 2007. p. 193–214.
- Kapuangan C, Soenarto RF, Marsaban AHM. Respons kardiovaskular pada laringoskopi intubasi: Perbandingan antara esmolol 100 mg dengan lidokain 1.5 mg [thesis]. Jakarta: Universitas Indonesia; 2008. p. 1–5. Indonesian.
- Kanchi M, Nair HC, Banakal S, Murthy K, Murugesan C. Haemodynamic response to endotracheal intubation in coronary artery disease: direct versus video laryngoscope. Indian J Anesth. 2011;55(3):260–5.
- Rosenblatt, WH. Airway Management In: Barash PG, Cullen BF, Stoelting RK, editors. Clinical Anesthesia. 5th Ed. Lippincot & Wilkins. Philadelphia;2006. p. 595–643.
- Thomas EBM, Moss S. Tracheal intubation. Anesth and Intens Care Med.2014;15(1):5–7.
- Butterworth IV JF, Mackey DC, Wasnic JD, editors. Airway management. In: Morgan and Mikhail’s clinical anesthesiology. 5th Ed. New York: Lange; 2013. p. 308–41.
- Aziz M. The role of video laryngoscopy. Adv in Anesth. 2013;31:87–98.
- Niforopulou P, Pantazopoulos I, Demestiha T, Koudouna E, Xanthos T. Video-laryngoscopes in adult: A topical review of the literature. Acta Anesthesiol Scand. 2010;54(9):1050–61.
- Charters S, Charters P. Alternative techniques for tracheal intubation. Anesth Intens.2014;15(5):209–14.
- Dominguez-Roldan JM, Barrera-Chacon JM, Murillo- Cabezas F, Santamaria-Mifsut JL, Rivera-Fernandez V. Clinical factors influencing the increment of blood carbon dioxide during the apnea test for the diagnosis of brain death. Transplantation Proceeding. 1999;31:2599–600.
- Murphy MF, Barker TD, Schneider RE. Endotracheal intubation in: Wals RM, Murphy MF, editors. Manual of emergency airway management. 3rd ed. Lippincot Williams & Wilkins. Philadelphia; 2008. p. 63–75.
- Rosenquist RW, Vrooman BM. Chronic pain management. In: Butterworth IV JF, Mackey DC, Wasnic JD, editors. Morgan and Mikhail’s clinical anesthesiology. 5th Ed. New York. Lange; 2013. p. 1023–85.
- Lubenow TM, Ivankovich AD, Barkin R. Management of acute postoperative pain. In: Barash PG, Cullen BF, Stoelting RK, editors. Clinical Anesthesia. 5th Ed. Lippincot & Wilkins. Philadelphia; 2006. p. 1405–40.
- Noppens RR, Geimer S, Eisel N, David M, Piepho T. Endotracheal intubation using the C-MAC® video laryngoscope or the macintosh laryngoscope: A prospective, comparative study in the ICU. Crit Care. 2012;16(3):1–8.
- Anonymous. Video intubation systems in storz the world of endoscopy. 5th ed. Tuttlingen: Karl Storz Corp; 2012. p. 61–3.
- McElwain J, Malik MA, Harte BH, Flyn NM, Laffey JG. Comparison of the CMAC® video laryngoscope with the macintosh, glidescope®, and airtraq® laryngoscope in easy and difficult laryngoscopy scenarios in manikins. Anaesthesia. 2010;65(5):483–9.
- Kovac AL. Controlling the hemodynamic response to laryngoscopy and endotracheal intubation. J Clin Anaesth. 1996;8(1):63–79.
- Kautto UM. Attenuation of the circulatory response to laryngoscopy and intubation by fentanyl. Acta Anaesthesiol Scand. 1982;26(3):217–21.
Copyright @ 2017 Authors. This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original author and source are properly cited.
mji.ui.ac.id