Section Abstract Introduction Methods Results Discussion Conflict of Interest Acknowledgment References
Community Research
Compliance in doing Senam Kesegaran Jasmani 1988 exercise improves cardiorespiratory endurance of attention deficit/hyperactivity disorder children
pISSN: 0853-1773 • eISSN: 2252-8083
https://doi.org/10.13181/mji.v27i1.1745 Med J Indones. 2018;27:44–53
Received: December 28, 2016
Accepted: March 19, 2018
Author affiliation:
1 Department of Community Medicine, Faculty of Medicine, Universitas Indonesia, Jakarta, Indonesia
2 Department of Child Health, Faculty of Medicine, Universitas Indonesia, Jakarta, Indonesia
Corresponding author:
Listya T. Mirtha
E-mail: tresnanti.listya@ui.ac.id
Background
Physical exercise was hypothesized to be able to improve the behavior of children with attention deficit/ hyperactivity disorder (ADHD) by improving attention and concentration. Several studies mentioned that physical exercise could make ADHD children calmer, not only as a supportive therapy, but also as a therapeutic therapy. The aim of this study was to evaluate the effects of physical exercise to the behavior of ADHD patients and to analyze the effects of Senam Kesegaran Jasmani 1988 (SKJ 88) exercise compliance to the cardiorespiratory endurance in ADHD children.
Methods
This study was an experimental study with 40 subjects from a special needs school in Tangerang, Indonesia. Subjects were given SKJ 88 exercise for 8 weeks, and the level of cardiorespiratory endurance was assessed with 600 m run before and after intervention.
Results
21 subjects (52.5%) were compliant, and the rest were very compliant. Although statistical analysis showed that there was no significant difference in cardiorespiratory endurance before and after intervention, the mean results of cardiorespiratory endurance test before intervention was higher than after. Mean time spent in the 600-m run before intervention was 497.9 seconds (SD 73.53), and after intervention was 313.7 seconds (SD 43.28).
Conclusion
Based on the statistical test, we concluded that there was significant decrease of time spent for cardiorespiratory endurance test (p<0.001). The reduction of time taken to run 600 m by 184.3 seconds (SD 73.33) showed the improvement of cardiorespiratory endurance after the treatment.
Keywords
children with ADHD, physical exercise, cardiorespiratory endurance
The prevalence of attention deficit and hyperactivity disorder (ADHD) has increased over the years, from 2–4 per 10,000 children 10 years ago to 15–20 per 10,000 children last year.1 The cause of this disorder remains unknown, but several studies has mentioned about the use of physical exercise as supportive therapy or even as therapeutic therapy in the replacement of pharmaceutical therapy. ADHD is a chronic neurobehavioral abnormality that causes changes in behavioral inhibition, has an efficient functioning in aim-oriented activity, or performs activity regulation according to the appropriate development stage. Disturbance in behavioral inhibition is also known as impulsivity, whereas an inability to function efficiently to fulfill aims is called inattention. Moreover, hyperactivity is a failure to regulate activity according to age.2
Senam Kesegaran Jasmani 1988 or often abbreviated SKJ 88 is a form of physical exercise that was popular in Indonesia during the new order governance. It was first introduced in 1984 (SKJ 84) according to Indonesian Presidential Decree No. 17/1984 on Jam Krida Olahraga.3 During that time, Indonesian government had a slogan “To exercise the general public and to publicize exercise” (mengolahragakan masyarakat dan memasyarakatkan olahraga) in order to increase the quality of human resources in Indonesia. It is believed that exercising regularly can increase physical and spiritual health. To show seriousness in increasing the interest of physical exercise across the country, the Minister of Youth and Sports at that time, Abdul Gafur, socialized a form of exercise that was obligatory every morning for elementary students to government officers. SKJ 88 was another form of exercise that was developed and improved from the exercises that has been introduced before. The implementation was set by the Decree of the Minister of Youth and Sports No. 0009/MENPORA/88, dated back to July 7, 1988.3
Based on the characteristics, SKJ 88 is a type of cardiorespiratory endurance exercise consisting of simple and easy-to-follow movements that can be performed by anyone, dynamic, cheerful, safe, and accompanied by music in the process. This form of exercise can be done individually or in small groups. For younger children, this exercise can give them opportunity to socialize with peers and the environment during their growth and development period. In addition, the movement in SKJ 88 also involves movements of the large muscle groups of the upper limb (biceps, triceps, deltoid), lower limb muscles (quadriceps, hamstring, gastrocnemius), and trunk muscles (abdominal and back).4
One of the components of physical exercise is cardiorespiratory endurance which is the ability of the cardiorespiratory system to take oxygen and distribute it to the whole body especially in the tissue that is currently active in the metabolism process.5,6 Physiological responses of physical exercise in children affects the cardiovascular system, respiration, blood circulation, and musculoskeletal. Volume of maximal oxygen uptake (VO2max) is commonly used as cardiorespiratory endurance measurement. VO2max increases as the age increases, reaching maximum VO2max at 18 years old for boys and 14 years old for girls.
One of the non-pharmaceutical therapy in children with ADHD is behavioral modification and play therapy followed with rhythmic movements. Being simple, easy to follow, with music companion, SKJ 88 has the potential to be a physical exercise option for ADHD. Based on this thought, SKJ 88-exercise, which is a cardiorespiratory endurance exercise model, is expected to provide positive benefits when performed by ADHD children because it combines elements of moving, practicing, playing, and music in its process. The aim of this study was to analyze the effects of SKJ 88 exercise compliance to the changing of cardiorespiratory endurance in ADHD children.
METHODS
This study used experimental research design, namely the pretest and posttest design, by giving routine SKJ 88 exercise to the subject.7, 8 The study was conducted at Sekolah Khusus Al-Ihsan Tangerang for 8 weeks, from 31st October until 23rd December, 2011. Study participant fulfilled the inclusion and exclusion criteria for this study and finished the treatment until the end. Exercise compliance was the ability of the participant to come and perform SKJ 88 exercise properly in the school. The benchmarks used were the number of participant’s attendance and the ability to do SKJ 88 exercise. The required forms were filled by instructor in charge of SKJ 88 exercise. Total attendance was assessed based on the recordings, while the assessment of exercise when performed was based on the checklists. Initially, the level of participants’ compliance in SKJ 88 exercise was grouped into non-compliant and compliant. However since there was a discrepancy, we made an adjustment based on the data distribution cutoff and changed the grouping into compliant and very compliant. Compliant was attendance less than cut-off value of total attendance, and total score on the checklist of exercise assessment over 8 weeks was less than the new cut-off. Very compliant was attendance more than or equal to the cut-off value of total attendance, and total score on the checklist of exercise assessment over 8-week period was more than or equal to the new cut-off value. Level of children’s cardiorespiratory endurance was measured using 600-meter run test.
Participants, environment, and study officers in this study were prepared before the cardiorespiratory endurance measurement. Participants preparation included: 1) sleeping adequately (at least 7 hours) on the night before the examination; 2) not performing heavy physical activity that caused fatigue the day before the examination; 3) not smoking nor drinking coffee or alcohol 3 hours before the examination; 4) having last meal 2 hours before the examination; 5) wearing sports clothing that absorbed sweat and comfortable to move in; 6) wearing comfortable shoes according to the test performed. Study preparation included: 1) health officer/non-health officers to act as: a. field officer (5 people), being in charge of cardiorespiratory endurance test (give start cue, timing, record the results), b. instructor (4 people), giving SKJ 88 exercise, c. medics (5 people), helping researcher when performing physical examination; 2) preparation of the test equipment and facilities as follows: a. cardiorespiratory endurance measurement test such as a running track, stopwatch, start flag, whistle, stationery to record the results, form, race number, b. physical, growth and development examination equipment such as stethoscopes, stature meter, digital scales, body fat analyzer, sphygmomanometer, results form, and stationery to record the results; 3) identifying participants, explaining and giving examples to correctly do examination; 4) using behavioral modeling, prompting and reinforcement for study participant to be comfortable. Preparation of the environment included: 1) endurance test done at the field started at 07.00 am; 2) physical examination conducted indoors, in a quiet room, using air conditioner maintained at a temperature of 21–25°C. After the preparation, participants began to follow the study protocol.
Stage of examination
This study consisted of three stages of the examination. Stage I examination was done before the participant performed cardiorespiratory exercise: 1) filling out the study forms by parents, which included name, age, date of birth, gender, address, occupation of parents, and parents’ income; 2) data input of participant’s physical activity by parents, with a total scoring of physical activity was performed by the physician; 3) filling the checklist of ADHD diagnosis according to DSM-IV TR criteria to determine the type of ADHD by pediatrician; 4) physical and motoric growthdevelopment examination of participant by researcher; 5) cardiorespiratory endurance test of participant using 600-meter run test conducted by an instructor. This stage was conducted a day after step number 1 to 4.
The 600-meter run test began with preparation such as blood pressure, breathing, and pulse measurement in a sitting position. Participants warmed up with stretching quadriceps, hamstring, gastrocnemius, that were held for 10 counts per movement together with the instructor. The participants were instructed to run towards the finish line with a total distance of 600 meters. Participants stood behind the start line. After the command “ready”, participant took a stand start and prepared to run. After hearing the whistle and seeing the flag raised by the officer, the participant ran to the finish line. Verbal encouragement from study officers were allowed during the test. Time was recorded from the time the whistle sounded until the participant crossed the finish line. Participants were considered failed if they did not successfully complete the required distance. After the run, participants underwent cooling of the quadriceps muscles, hamstring, gastrocnemius, with stretching exercises 10 counts per movement. After cooling period, the measurement of blood pressure, breathing, and pulse was repeated in sitting position.
Stage II examination was the period of examination when the participants did SKJ 88 exercise for 8 minutes 38 seconds in two sessions a day at school (before starting lessons at school and before going home) 5 days a week. The goal was to assess compliance (presence and ability to conduct) of SKJ 88 exercise, cardiorespiratory endurance test, and participant’s behavior during the study. In this stage, the instructor filled the attendance form and compliance checklist of SKJ 88 exercise. Evaluation during the 8-week period included: 1) measurement of participant’s cardiorespiratory endurance using 600-meter run test conducted by the instructor; 2) recorded complaints that the participants had during the run.
Participant selection used non-probability sampling with consecutive sampling method. All children with ADHD that met the selection criteria were included in the study.9 Inclusion criteria were as follows: a) boys and girls aged 6–12 years; b) diagnosed ADHD by a physician; c) attending Sekolah Khusus Al-Ihsan (Al-Ihsan Special-Needs School) in the academic year of 2011/2012, (d) were not using drug for ADHD of for at least one month; e) did not participate in structured physical activity; f) joined routine physical exercise for less than 3 times a week; g) having no contraindications to perform physical exercise; h) having parents’ consent by signing the form. Participants were excluded if: a) having previous musculoskeletal injuries or worsened symptoms that caused contraindication to do exercise; b) not having parent’s consent to participate in the study. The sample size used in the study was calculated using sample size equation for analytical research formula and the results of numerical pairs 34 people. To anticipate the drop out, an additional 15% was added to the total participants needed, which were 5 people in total.7,8 Thus, the minimum required sample size were 39 people. Nevertheless, the number of participants that joined this study were limited to the number of student that met the inclusion criteria.
The collected data were then analyzed as follows: 1) descriptive statistics to determine the physical and socio-demographic characteristics, based on the mean and standard deviations. Results were presented in tabular and written form, adapted to the scale and distribution data; 2) data recapitulation of SKJ 88 exercise compliance and analysis on each compliance indicators using one-sample t test. Data were analyzed to determine differences between the study participants’ behavior before and after the treatment with paired t test. Normality test was done using Shapiro Wilk test since the number of study participants were less than 50. P value <0.05 was considered statistically significant; 3) cardiorespiratory endurance analysis before and after exercise during the 8 weeks’ intervention period were done using paired t test; 4) ANOVA test to compare cardiorespiratory endurance between the compliant and very compliant group. Post-hoc Bonferroni analysis were also conducted to determine the effects of SKJ 88 exercise compliance to the changes in cardiorespiratory endurance after intervention. This study had received approval from the Research Ethics Committee of the Faculty of Medicine of Universitas Indonesia with the permission of ethics number 554/PT02.FK/ETHICS/2011. Informed consent was received from parents of study participants after receiving explanation about the intervention.
RESULTS
The physical and socio-demographic characteristics of study participant
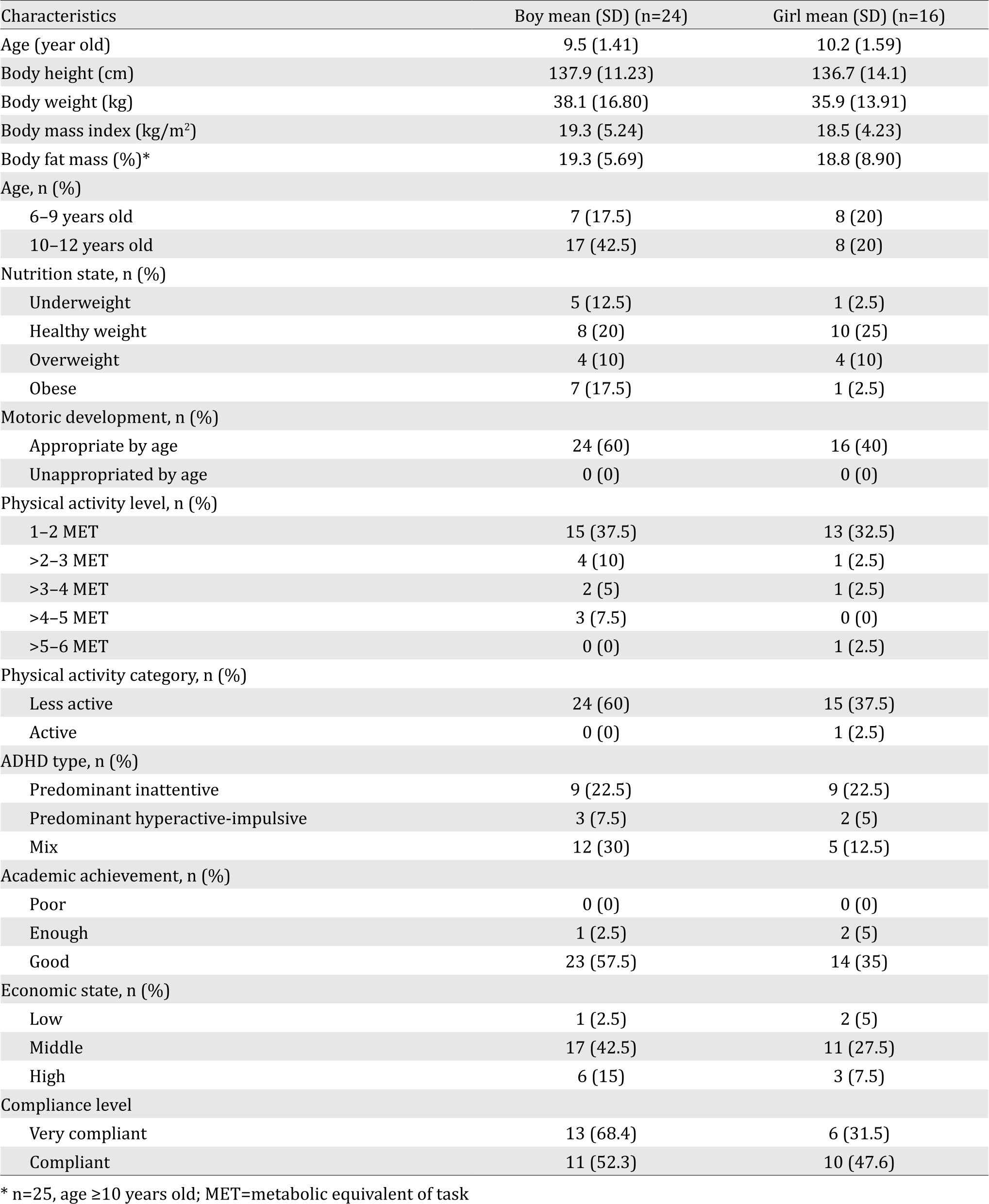
Table 1 shows the physical and sociodemographic characteristics of study participants. The mean age of the participants were 9–10 years old that had motoric development in accordance to the age of the participant. Most participants (18 children) had healthy nutritional status. 70% of the subjects had a physical activity level 1–2 metabolic equivalent of task (MET). The majority (97.5%) of participants were categorized as less active in the physical activity category. Greater number of the participant had ADHD category of predominant inattention (45%) (Table 1).
Table 1. Physical and sociodemography characteristics of study subjects
Attendance absentee pattern changes
Based on the pattern of participant’s attendance in the fourth and eighth week, there was an increase on the average attendance by 2.6 days (SD 1.99). Statistical analysis showed a significant increase (p<0.001) in the participant attendance. Total attendance of participant for the period of 8 weeks at 90.9% (SD 5.42), and using the cut-off value of the median showing the attendance of the participants had exceeded 90%. From the adjustment, it was obtained that 29 subjects were very compliant, and the rest was compliant.
Compliance of Subject Research Based on Ability Doing SKJ 88 Exercise
The increase of the mean score was 27.5 days (SD 12.03). Statistical analysis showed a significant increase (p<0.001) on the ability of the subject doing SKJ 88 exercise. Compliance subjects were measured both in quantity and quality for a success rate of research. Indicators quantity of this treatment was the absence of presence, while the ability to do SKJ 88 exercise was an indicator of the quality of treatment. In this study, the subject was said to be “very comply” if it had met compliance in quantity and quality, so only did grouping that contained a subject that really met compliance in quantity and quality. Instead, the subject was said to be “comply” if it did not meet one compliance.
The subject compliance based on attendance and ability doing SKJ 88 exercise
Participants compliance were measured both in quantity and quality to assess the success rate of the study. Quantity indicators of the intervention were based on the attendance, while the ability doing SKJ 88 exercise was a quality indicator of intervention. In this study, the participants were considered as “very compliant” if they had met the compliance criteria both quantitatively and qualitatively. Therefore, the group only consisted of participants that were compliant both in quantity and quality. Conversely, participants that were compliant did not comply either quantitatively or qualitatively. Based on the predefined grouping and adjusted distribution of data, 19 subjects were very compliant, and the rest was compliant for the intervention. Compared to previous results, compliance of 10 subjects only increased in quantity, but not in the quality after intervention for 8 weeks.
Cardiorespiratory endurance level
From the test results, the cardiorespiratory endurance level was obtained. Statistical analysis showed that there was no significant difference between the level of cardiorespiratory endurance before and after intervention. However, the running time spent on the cardiorespiratory endurance tests showed that the result prior to treatment was 497.9 seconds (SD 73.53) and after treatment was 313.7 seconds (SD 43.28). Based on the statistical analysis, the decrease of time results in cardiorespiratory endurance time tests were significant (p<0.001), with a mean difference of 184.3 seconds (SD 73.33). Hence, it could be concluded that there had been an improvement of cardiorespiratory endurance in participants after intervention (Figure 1).
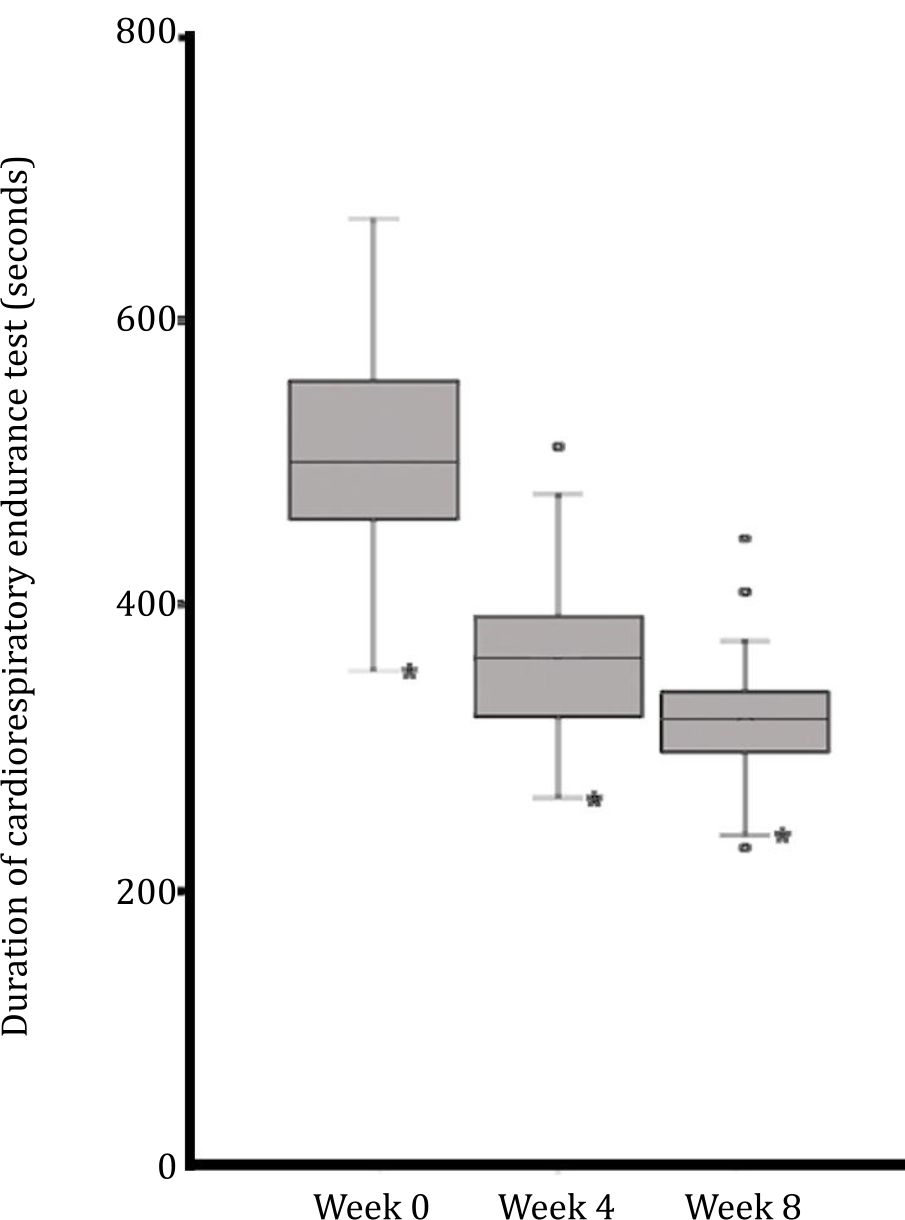
Figure 1. Cardiorespiratory endurance during SKJ 88 exercise. There was a tendency of improving of endurance after the intervention (* p<0.05)
Effects of SKJ 88 exercise compliance towards cardiorespiratory endurance changes
Shapiro Wilk normality test showed normal distribution of the cardiorespiratory endurance test results. Cardiorespiratory endurance was improved after intervention in both group of very compliant and compliant participants. Statistical analysis showed that SKJ 88 exercise compliance was significantly different (p<0.001) in improving cardiorespiratory endurance in both participant in very compliant and compliant groups. In addition, there were a significant improvement in the cardiorespiratory endurance (p<0.001) in both groups at each measurement although the results of post hoc Bonferroni showed no significance difference between compliant and very compliant group at each measurement. Nevertheless, the mean difference between before and after intervention were greater in the very compliant group.
DISCUSSION
One of the inclusion criteria in selecting study participant was based on DSM-IV that mentioned ADHD were frequently found in primary school children. Thus, the age range of the participant were 6–12 years old.2 Several children (14/40) who studied at Sekolah Khusus Al-Ihsan already passed primary school phase, but in the process, they received rejection from the school environment and moved to other school. SKJ 88 exercise is one of the non-pharmaceutical therapy in children with ADHD by modified behavioral and play therapy followed with rhytmic movement. The most significant increase could be seen after doing SKJ 88 exercise was improving cardiorespiratory endurance and behavior after the treatment. SKJ 88 exercise was used as an intervention in this study which was given as a mandatory part of the learning activities in the school. This is a lucrative opportunity to introduce forms of physical activity in children with ADHD at school as well as an effort to maintain the continuity of the implementation and to reduce the risk of participant’s non-compliance during the study. Remembering that ADHD children has low motivation to participate in physical exercise, it is necessary to give chance to ADHD children to participate in physical exercise to improve physical fitness and motoric ability.
In this study, participants’ compliance was assessed from two aspects, namely the attendance and the ability of doing SKJ 88 exercise. Both showed significance results. From the attendance, significant improvement was seen from 1) increase attendance of participants in the school beginning from the fourth week of intervention; 2) decrease number of absence in school due to illness beginning from the fourth week of intervention until the eighth week. Meanwhile from the aspect of ability doing SKJ 88 exercise, the most significant changes could be seen from 1) increased ability along with interest of participants in doing SKJ 88 exercise with more enthusiasm and by being more active after merely seeing their peers doing SKJ 88; 2) increased in participants’ ability in terms of skills in coordinating the movement in accordance with the movement exemplified by the instructor.
SKJ 88 exercise was carried out every day in school with an instructor giving larger visual instruction compared to verbal instruction and with constant supervision during the whole exercise process. This was done in accordance to the recommendations of physical exercise for children issued by American College of Sports Medicine (ACSM). In order to ensure the security of the physical exercise implementation in children, proper instruction should be given, and exercise should be supervised.10 In addition, to anticipate boredom that might occur during the study and to make sure the participant were able to do the exercise, the SKJ 88 exercise was carried out in two practice sessions, before school started and before participants returned home, with each session lasted for 8 minutes 38 seconds. The total time spent for SKJ 88 exercise in a day was 17 minutes 16 seconds, so that the energy source during this exercise was about 80% from aerobic energy sources and the remaining 20% anaerobic.11 Thus, SKJ 88 exercise in this study was a form of exercise for cardiorespiratory endurance.
In the beginning of this study, simulations were conducted in advance for all matters related to the whole study and also for the participants, parents, and teachers at school. SKJ 88 song used during the exercise was played in the school for 1 month before the study was conducted to see the participants’ response when they heard the song. From the first time SKJ 88 music being played in the school, no rejection was given by the participants. The participants’ parents who initially felt anxious and was afraid of the intervention given, finally gave permission for the children to join SKJ 88 exercise. Parents’ participation could also be seen from their companion to the participant every Friday by joining the SKJ 88 exercise. This was in accordance to Cairney et al's research, that another form of treatment for ADHD children was by giving physical activity that was likeable and doable, with movements that could be easilytrained. Hence, there would be an increase in persistence for the activity.6 The hope was that participation would increase along with the process of adaptation from all parties involved, as well as the establishment of compliance towards physical activity.
Several factors played role in the compliance of the participants in doing SKJ 88. Socialization of the SKJ 88 implementation influenced subject compliance. SKJ 88 has simple movements with a pleasant musical companion that could be a factor of interest shown in the participants in performing SKJ 88 every day at school, which then could be performed at home without help by several participants. This independence began to appear on the participant from the fourth week of SKJ 88 exercise implementation. The most important thing that played an important role was the support of parents and teachers who patiently helped in the form of verbal encouragement to the participants while doing exercises SKJ 88 since the introduction period. They made the participants more excited and motivated in doing the SKJ 88 exercise. During the exercise period, behavioral modification was given to participants in form of modeling, prompting, and reinforcement.
Previously mentioned, a child could experience improvement in cardiorespiratory function after doing physical exercise although it was not the same as adults. In this study, participants showed very low level of cardiorespiratory endurance. This result was consistent with the findings from Wu et al., where there was low cardiorespiratory endurance in children with coordination difficulties in Taiwan.12 In other words, subjects in this study had a risk of low physical fitness, causing reciprocal effects to the motor skills and participation in physical exercise.
In this study, cardiorespiratory endurance test that were used was a form of field tests as previously conducted in other studies.12–14 Measurement of cardiorespiratory endurance using field tests (sub-maximal test) were easier to conduct compared with laboratory tests (maximum test). The cardiorespiratory endurance tests required the participants’ ability to receive instruction, to coordinate, to cooperate, and to have high motivation. This had become one of the difficulties for the participants in this study. Similar to cardiorespiratory endurance exercise test conducted by Tamin TZ15 in children with intellectual disability (ID), the study encountered some hindrance associated with the participants’ disorder and the limitations while taking cardiorespiratory endurance measurement. Several obstacles encountered in this study during 600-meter run test simulation in athletics track at Sekolah Ragunan were participants’ lack of motivation and attention, participants’ low motoric skills, and participant’s discomfort due to track width and the hot weather. This was not in accordance with the special consideration given for physical exercise in children as issued by ACSM. Implementation of physical exercise in children should be performed in an environment with a neutral temperature and should always pay attention to the hydration factor for body since the temperature regulation in children were still immature.16 In addition, the large area of the place caused difficulties for officers and teachers to monitor and control the subject.
This study showed a significant improvement in time spent for cardiorespiratory endurance test after intervention were given regardless of whether cardiorespiratory endurance level changes were significant or not. It took an average of 497.9 seconds for the participants to run 600 meters before the treatment, and the average time decreased to 313.7 seconds after 8 weeks of intervention. The test time reduction showed an improvement of cardiorespiratory endurance. Hence, it can be assumed that there had been a process of adaptation from doing SKJ 88 exercise, which was a simple form of cardiorespiratory endurance exercise.
The downward trend in the mean time in the fourth week of treatment in this study was an acute response to workouts. As mentioned before, to cause an acute response from children, a higher intensity physical activity is required.17 Most participants were classified as having low physical activity, causing SKJ 88 exercise implementation led to an acute response in their body. Meanwhile, after the eighth week of intervention, the process of adaptation in their body had begun. This was indicated by several participants in the study felt the need to replay SKJ 88 music after the exercise had finished to redo the exercise from the fourth week. Similarly, parents of participants told the researcher that the participant tried to do the SKJ 88 exercise by their own, so that they felt the need to buy their own SKJ 88 music to accompany their children exercising at home. This indicates that evaluation of the exercise program given to ADHD children is needed at the eight week.
In addition, parents had also reported that doing SKJ 88 exercise routinely at schools made the children healthier and less susceptible to disease even though the surrounding were sick. This is proven by a decreased in the number of student absent from school due to illness. The range of 0-6 days of absence due to illness in the first 4 weeks (with an average of 1-4 days) was reduced to 0-1 days in the second four weeks (with an average of 1 day). It was also acknowledged that children did not get tired easily in daily life, which made them more vibrant in activity. These results were in line with the findings of Baxter-Jones and Tolfrey, which stated that providing aerobic exercise for children to improve their physical fitness level is beneficial for physical performance and its relationship to health. It will provide improvements in cardiorespiratory endurance by 5%.17 This study showed an improvement of cardiorespiratory endurance travel time by 37% after treatment for 8 weeks.
In this study, both very compliant and compliant groups equally improved cardiorespiratory endurance and behavior after the treatment. In other words, compliance became a major factor for changes in cardiorespiratory endurance and behavior of ADHD children through the provision of physical exercise even though the hypothesis of this study was not proven. This was because all subjects were in the same compliant group before adjustments were done. The adjustments were performed by using clustering differentiation with cut-off value based on the distribution of new compliance data obtained, in which the value was high enough.
In this study, compliance was established from the beginning of the study and was not there from the start before SKJ 88 exercise implementation. The results in this study showed an increase in compliance both in quantity and quality aspects, along with the improvement of cardiorespiratory endurance and the participants’ behavior. The compliant group showed improvement of travel time in cardiorespiratory endurance test after 8 weeks of treatment, although not as fast as in the very compliant group. Interestingly, teachers saw more improvements in the compliant group. In other words, participants who were compliant showed more behavioral improvement in school. This showed that the participants’ behavior could be different between at school and at home, so the observation of behavior was still required at both places and cannot represent each other.
This study reported that compliance of doing SKJ 88 exercise influence cardiorespiratory endurace of ADHD children which was marked by reduced time spent while doing run test as cardiorespiratory endurance test in both compliant and very compliant group. However, the very compliant group had better cardiorespiratory endurance test result than the compliant group. Additionally, the study showed that compliance doing SKJ 88 exercise influenced the improvement of behavior at home and school in both very compliant and compliant group which assessed by SPPAHI parent (SPPAHI-O/ Skala Penilaian Perilaku Anak Hiperaktif-Orangtua) and SPPAHI teacher (SPPAHI-G/ Skala Penilaian Perilaku Anak Hiperaktif-Guru).18
In conclusion, this study showed the improvement of cardiorespiratory endurance after intervention of SKJ 88 exercise. Improvement pattern of cardiorespiratory endurance of the subject appeared on the fourth week, which gradually decreased until the eight week. The authors suggest this exercise to all ADHD children and recommend it as a part of physical education subject in school. SKJ 88 exercise may be used as a supplementary therapy to improve cardiorespiratory endurance of ADHD children. Moreover, further research is warranted such RCT design by adding external comparison group to prove the association between compliance by doing SKJ 88 exercise and cardiorespiratory endurance.
Conflicts of Interest
The authors affirm no conflict of interest in this study.
Acknowledgment
We thank Jull Kurniarobbi, MD. Sports Med. for his general support to this article. In addition, we thank all teachers and staff of Sekolah Khusus Al-Ihsan, Tangerang, Indonesia for their sincere help and encouragement.
REFERENCES
- Delphie B. Pendidikan Anak Autistik. Edition 1. Sleman: KTSP; 2009. Indonesian
- Paternote A, Buitelaar J. ADHD – Attention Deficit Hyperactivity Disorde (Gangguan Pemusatan Perhatian dan Hiperaktivitas), tanda-tanda, diagnosis, terapi, serta penanganannya di rumah dan di sekolah. Edition 1. Jakarta: Prenada; 2010. p. 110–20. Indonesian.
- Departemen Pemuda dan Olahraga RI. Petunjuk pelaksanaan Senam Kesegaran Jasmani. Buletin Departemen Pemuda dan Olahraga RI; 1988. Indonesian.
- American College of Sports Medicine. Guidelines for exercise testing and prescription. 7th ed. Baltimore : Lippincott Williams & Wilkins. 2006. p. 237–45.
- Nieman DC. Physical fitness defined. In: Barrosse E, editor. Exercise testing and prescription. 6th ed. Iowa : Mc Graw Hill Companies. 2007. p. 30–43.
- Departemen Kesehatan RI. Petunjuk teknis pengukuran kebugaran jasmani. Buletin Departemen Kesehatan RI; 2005. Indonesian.
- Saputro D. ADHD (Attention Deficit/Hyperactivity Disorder). Print 1. Jakarta: Sagung Seto; 2009. Indonesian.
- Dwayer T, Sallis J, Blizzard L, Lazarus R, Dean K. Relation of Academic Performance to physical Activity and Fitness in Children. Pediatr Exercise Science. 2001;13:225–38.
- American Academy of Pediatrics Committee of Quality Improvement Subcommittee on Attention-Deficit/ Hyperactivity Disorder. Clinical practice guideline: Treatment of the school-aged child with attention deficit/hyperactivity Disorder. Pediatrics. 2001; 108(4):1033–44.
- Centers for Disease Control and Prevention [Internet]. Attention-Deficit/Hyperactivity Disorder (ADHD). 2010 [cited Des 26, 2010]. Available from: http://www.cdc. gov/ncbddd/adhd/conditions.html.
- Cahyani N. Latihan jasmani untuk anak-anak. In: Indonesia sehat, Indonesia bugar – Seri latihan jasmani untuk perempuan dan anak-anak. Jakarta: Balai Penerbit FKUI; 2008. p. 34–48. Indonesian.
- Cairney J, Hay JA, Faught BE, Flouris A, Klentrou P. Developmental coordination disorder and cardiorespiratory fitness in children. Pediatric Exercise Science [Internet]. 2007 [cited Des 26, 2010]; 19:20- 8. Available from: http://www.ncbi.nlm.nih.gov/ pubmed/17554154
- Wu SK, Lin HH, Li YC, Tsai CL, Cairney J. Cardiopulmonary fitness and endurance in children with developmental coordination disorder. Res Dev Disabil. 2010;31(2):345–9.
- Tsai CL, Chen WEI, Li YC, Wu SK. Physical fitness in children with developmental coordination disorder. Health Promotion Science. 2006;1:25–37.
- Tamin TZ. Model dan efektivitas latihan endurans untuk peningkatan kebugaran penyandang disabilitas intelektual dengan obesitas [Disertasi]. Jakarta: Medicine Faculty of Universitas Indonesia; 2009. Indonesian.
- Kaplan-Liss E, Renna ME. Exercise in children “Exercise is a family affair”. In : Jonas S, Phillips EM, editors. ACSM’s exercise is medicine: A clinician’s guide to exercise prescription. USA: Lippincott Williams & Wilkin. 2009; p. 230–44.
- Matos N, Winsley RJ. Trainability of young athletes and overtraining. J Sports Sci Med. 2007;6(3):353–67.
- Mirtha LT. Pengaruh Kepatuhan Latihan Senam Kesegaran Jasmani 1988 Terhadap Perilaku Anak dengan Gangguan Pemusatan Perhatian/Hiperaktivitas. Sari Pediatr. 2016;18(2):147. Indonesian.
Copyright @ 2018 Authors. This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original author and source are properly cited.
mji.ui.ac.id