Case Report
Acanthamoeba keratitis: a challenge in diagnosis and the role of amniotic membrane transplant as an alternative therapy
pISSN: 0853-1773 • eISSN: 2252-8083
https://doi.org/10.13181/mji.v27i4.2007 Med J Indones. 2018;27:299–303
Received: May 22, 2017
Accepted: October 22, 2018
Author affiliation:
Department of Ophthalmology, Faculty of Medicine, Universitas Indonesia, Cipto Mangunkusumo-Kirana Hospital, Jakarta, Indonesia
Corresponding author:
Ratna Sitompul
E-mail: ratna_sitompul@yahoo.com
Acanthamoeba keratitis (AK) is a very rare, sight-threatening corneal disease caused by the infection of a free-living amoeba. The aim of this report was to demonstrate the challenges in the diagnosis of AK with an atypical presentation. Amniotic membrane transplantation (AMT) was done in this case to accelerate wound healing. A woman who frequently used contact lens came with redness and a whitish spot in her left eye 2 weeks before admission. There was a history of rinsing contact lens in tap water. The patient had already been on a topical steroid for 2 weeks. Visual acuity of the left eye was light perception with wrong projection. Examination of the left cornea showed a semi-circular central ulcer with a 5.8-mm area and 1/3 stromal depth. It is surrounded by a feathery-edge infiltrate with positive satellite lesions but without hypopyon. It was diagnosed as corneal ulcers due to mixed infection (bacteria and fungi). After 2 weeks of bacterial and fungal therapy, the size of the ulcer decreased, but the corneal infiltrate remained; therefore, an Acanthamoeba culture was done to determine the possibility of Acanthamoeba infection. Two weeks after the Acanthamoeba topical therapy, the visual acuity improved. AMT was performed to accelerate wound healing. Two months post-AMT, visual acuity improved to 1/60 with no conjunctival or ciliary vasodilation, and the ulcer was resolved. The patient was planned to undergo keratoplasty. The diagnosis of AK with an atypical presentation is challenging. AMT can be used as an alternative therapy to accelerate wound healing.
Keywords
Acanthamoeba keratitis, amniotic membrane transplantation, propamidine isethionate
Acanthamoeba keratitis (AK) is a very rare, sight-threatening corneal disease that results from the infection of a free-living amoeba.1–3 The estimated rate of AK is 1.2 per million people in the United States and 0.2–2 per 10,000 soft contact lens wearers per year in the United Kingdom.1 Acanthamoeba penetrates the eye through minimal corneal trauma, which usually occurs in individuals who routinely wear soft contact lenses.4 Patients with AK will experience pain and photophobia, and the infection runs progressively leading to corneal perforation if left untreated.2,5,6 Initial manifestation is characterized by a complete or partial ring infiltrate in the anterior stroma, which may respond well to steroid therapy.2,4 Atypical manifestations, such as diffuse punctate epitheliopathy, dendritic epithelial lesion, or feathery-edge lesion, are also observed in other cases of keratitis. Therefore, AK is often mistreated as herpes simplex virus keratitis or even fungal keratitis in common practice.2,4,6 The diagnosis of AK is often difficult as the manifestations could mimic other types of keratitis. Furthermore, its treatment is time-consuming; hence, a proper and accurate diagnosis is crucial. A delayed diagnosis could also lead to a delay in treatment, and the prognosis of the disease could worsen. Here, we present a challenging diagnostic and treatment process of a contact lens-associated infective keratitis case caused by Acanthamoeba, which was treated with antibiotics and amniotic membrane transplantation (AMT) to enhance the healing process.
Case Report
A 32-year-old woman came with chief complaints of redness and a whitish spot in her left eye since 2 weeks before admission. She complained of blurred vision and foreign body sensation without any significant pain. She had been using monthly disposable soft contact lenses for 1 year and regularly rinsed her contact lenses and case using commercial disinfectant solutions, but she also used tap water on many occasions. She went to a general practitioner and was treated with steroid ED four times daily without any improvements.
The visual acuity of the left eye was light perception with wrong projection and the right eye was 6/6 with correction. Examination of the left cornea showed a semi-circular central ulcer with a 5.8-mm area and 1/3 stromal depth, surrounded by a feathery-edge infiltrate and satellite lesions. The anterior chamber was deep with no hypopyon, and the other part was hard to evaluate (Figure 1).

Figure 1. The initial clinical appearance of the left eye showed a semi-circular central ulcer with an area of 5.8 mm with 1/3 stromal depth, surrounded by a feathery-edge infiltrate and satellite lesions
We diagnosed this patient with a corneal ulcer due to suspected mixed infection of bacterial and fungal microorganisms of the left eye. The cornea was scrapped, and potassium hydroxide (KOH) and Gram examinations were carried out, but the results were negative. The patient was treated with moxifloxacin ED hourly, natamycin ED hourly, and polymyxin, neomycin, and gramicidin (Polygran®) EO three times a day. After 2 weeks of treatment, the visual acuity improved to light perception with good projection. However, the central corneal ulcer size remained 3×4 mm with 1/3 stromal depth. Because of an inadequate response to treatment, voriconazole ED was added hourly, and a culture for Acanthamoeba was performed to find other etiologic agents. Two weeks after the procedure, a positive result was obtained from the Acanthamoeba culture. Hence, we changed the treatment to propamidine isethionate (Brolene®) ED and polymyxin, neomycin, and gramicidin ED hourly for the left eye. After 2 weeks of the Acanthamoeba treatment, visual acuity improved to hand movement with good projection. Scar tissue started to form, but the epithelial defect was still observed in the cornea, which indicated delayed healing of the lesion (Figure 2).
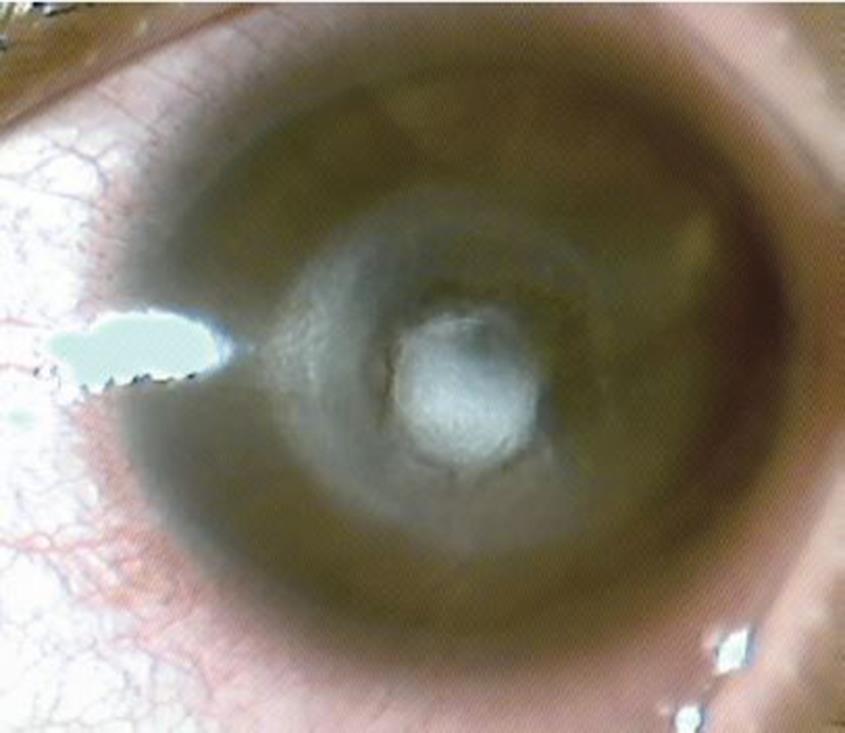
Figure 2. Two weeks after the Acanthamoeba treatment, scar tissue started to form
AMT was performed to accelerate the healing process of the ulcer after 6 weeks of treatment. The amniotic membrane has been used in ocular surface disorder as it acts as media for ocular surface growth and offers extensive antiinflammatory, antifibrosis, antiangiogenesis, and antibacterial properties, which eventually promote reepithelization. After surgery, treatment using propamidine isethionate ED and polymyxin, neomycin, and gramicidin ED was continued hourly for the left eye. Two months after AMT, visual acuity of the left eye gradually improved from hand movement with good projection to 1/60. Because of cicatrix in the central cornea, the patient was scheduled to undergo corneal transplantation until a corneal donor is available (Figure 3). The patient was informed and gave a consent for a publication.
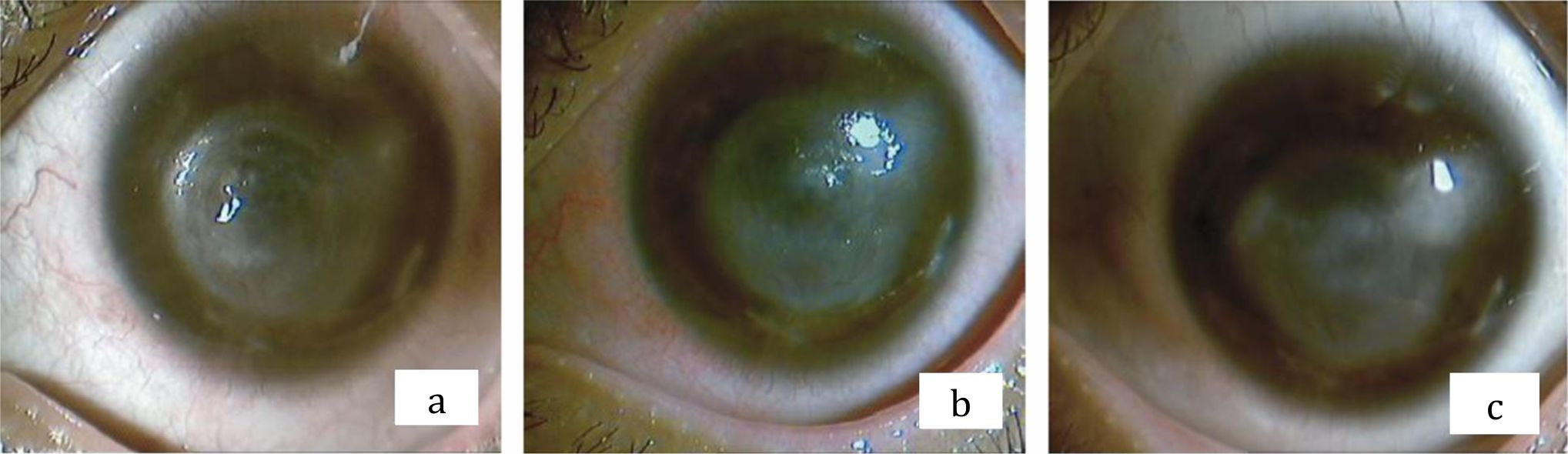
Figure 3. Clinical improvement of the left eye after the amniotic membrane transplantation procedure. (a) Two weeks after the procedure, there were no epithelial defects and infiltrate; (b) One month after, the central defect had been resolved and cicatrix formed; (c) Two months after, there was no conjunctival or ciliary vasodilation, and the ulcer resolved along with the corneal scar
DISCUSSION
Several studies reported the use of a soft contact lens as one of the greatest risk factors for corneal infection.2,7 However, a recent study by Jiang et al8 reviewed clinical characteristics of AK between 1991 and 2013. Out of the 260 cases included, it was revealed that the most common risk factor was ocular trauma (53.1%) and then followed by contact lens wear (29.8%). In Cipto Mangunkusumo Hospital, the most common etiologies of the corneal ulcer-related soft contact lens are bacterial (68%) and fungal (9.55). Only one case of AK was found in the past 5 years.9
In this case, the patient regularly rinsed her contact lenses and the case with commercial disinfectant solutions. However, she also frequently used tap water, which is known as one of the sources of Acanthamoeba. Acanthamoeba is found worldwide in air, dust, soil, and fresh waters, and it is relatively resistant to normal levels of chlorine in tap water.4
In addition, the patient had also rinsed her eyes using betel leaf water twice. This might have intoxicated the cornea and caused necrosis and corneal melting, which facilitated the penetration of Acanthamoeba. Betel leaf has been described from ancient time as an antiseptic for corneal infection. Piper betle Linn. infusion in 5%, 10%, and 20% concentrations were safe in a normal cornea, but it is toxic in a damaged cornea.10 Several risk factors were found in the patient such as using contact lens, rinsing contact lens on tap water, which is the source of Acanthamoeba, and taking a steroid, which decreases the corneal defense mechanism, hence increasing the pathogenicity of Acanthamoeba.2,3
However, the diagnosis of AK is often challenging as the manifestation may be similar to fungal keratitis or bacterial corneal ulcer; hence, further examination may be required. The patient was originally treated as mixed bacterial and fungal infection because of the risk factors, clinical manifestations, and epidemiology data that reveal that the most common etiologies of corneal ulcer are bacterial and fungal despite the negative result of Gram and KOH examinations. Other challenges lie in the confirmation of diagnosis as the gold standard examination is culture specimen inoculation in Escherichia coli-plated non-nutrient agar that requires 14 days to grow; therefore, it is considered difficult and time-consuming to grow Acanthamoeba on the disc. Acanthamoeba has two forms in its life cycle: trophozoite and cyst. The trophozoites are sensitive to most available chemotherapeutic agents (antibiotics, antiseptics, antifungals, antiprotozoal including metronidazole, antivirals, and antineoplastic agents).11 However, cysts are more difficult to eradicate, and only a few of these drugs are proven effective. Treatments that are regularly used as an antiamoebic agent are biguanides (e.g., polyhexamethylene biguanide and chlorhexidine), diamides (e.g., propamidine), and aminoglycosides (e.g., neomycin). Biguanides are the most potent drug to eliminate the cyst form of Acanthamoeba.2,12
A number of antimicrobial agents have been recommended for AK therapy based on their in vitro amebicidal effects as well as their clinical effectiveness. After the microbiology result, the patient was treated with propamidine isethionate ED and polymyxin, neomycin, and gramicidin ED. The biguanides interact with the cytoplasmic membrane, resulting in a loss of cellular components and inhibition of respiratory enzymes; thus, it has a cytocidal effect to Acanthamoeba.12 Even though diamidines also has a cytocidal effect, the drug is not available in Indonesia.
Two weeks after treatment, the left eye showed a moderate response to the treatment. Visual acuity improved from hand movement with wrong projection to hand movement with good projection. The size of the infiltrate in the central cornea was reduced, and the lesion was surrounded with cicatrix tissue. Vemuganti et al13 reported that in severe cases of AK, the cases that did not respond to adequate medical treatment should undergo surgical intervention.
In terms of treatment of AK, penetrating keratoplasty is the most common surgical procedure done by ophthalmologists. Unfortunately, because a corneal donor was unavailable, keratoplasty should be postponed. Because of progressive corneal inflammation and persistent epithelial defect in this patient, AMT was performed to control inflammation and accelerate the healing process while waiting for the corneal donor in order to execute keratoplasty.14 Frozen amniotic membranes were arranged layer by layer from the bottommost until it covered the depth of the ulcer. The amniotic membranes were then stitched to the cornea using 10.0 nylon and covered with bandage contact lens. The success rate of amniotic membrane use in corneal ulcer in Cipto Mangunkusumo Hospital is 90%.14 Final measurement on visual acuity showed significant improvement from light perception to 1/60.
In conclusion, the diagnosis of AK with an atypical presentation is challenging. AMT can be used as an alternative therapy to accelerate wound healing.
Conflicts of Interest
The authors affirm there is no conflict of interest in this study.
Acknowledgment
None.
REFERENCES
- Page MA, Mathers WD. Acanthamoeba keratitis: a 12-year experience covering a wide spectrum of presentations, diagnoses, and outcomes. J Ophthalmol. 2013;2013:670242.
- Clarke B, Sinha A, Parmar DN, Sykakis E. Advances in the diagnosis and treatment of Acanthamoeba keratitis. J Ophthalmol. 2012;2012:484892.
- Rahimi F, Hashemian SM, Tafti MF, Mehjerdi MZ, Safizadeh MS, Pour EK, et al. Chlorhexidine monotherapy with adjunctive topical corticosteroids for Acanthamoeba keratitis. J Ophthalmic Vis Res. 2015;10(2):106–11.
- Dini LA, Cockinos C, Frean JA, Niszl IA, Markus MB. Unusual case of Acanthamoeba polyphaga and Pseudomonas aeruginosa keratitis in a contact lens wearer from Gauteng, South Africa. J Clin Microbiol. 2000;38(2):826–9.
- American Academy of Ophthalmology. Infectious diseases of the external eye: microbial and parasitic infections In: American Academy of Ophthalmology, ed. External disease and cornea. San Fransisco: American Academy of Ophthalmology; 2011:167–4.
- Dart JK, Saw VP, Kilvington S. Acanthamoeba keratitis: diagnosis and treatment update 2009. Am J Ophthalmol. 2009;148(4):487–99.
- Sharma S, Garg P, Rao GN. Patient characteristics, diagnosis, and treatment of non- contact lens related Acanthamoeba keratitis. Br J Ophthalmol. 2000;84(10):1103–8.
- Jiang C, Sun X, Wang Z, Zhang Y. Acanthamoeba keratitis: clinical characteristics and management. Ocul Surf. 2015;13(2):164–8.
- Desrina, Susiyanti M. Profil Demografis, Karakteristik Klinis dan Evaluasi Hasil Terapi Ulkus Kornea Akibat Lensa Kontak di Divisi Infeksi Imunologi RSCM Kirana Periode Januari 2013–Desember 2014. Penelitian Deskriptif. Jakarta: Universitas Indonesia; 2015.
- Ariesta P, Sitompul R, Susiyanti M, Setiawati A, Mun’im A. Keamanan rebusan daun sirih (Piper Betle Linn) 5%, 10% dan 20% terhadap jaringan anterior mata normal pada kelinci percobaan [tesis]. Jakarta: Universitas Indonesia; 2007. Indonesian.
- Graffi S, Peretz A, Jabaly H, Naftali M. Acanthamoeba keratitis. Isr Med Assoc J. 2013;15(4):182–5.
- Wilson ME Jr, Trivedi RH, Buckley EG, Granet DB, Lambert SR, Plager DA, et al. ASCRS white paper. Hydrophobic acrylic intraocular lenses in children. J Cataract Refract Surg. 2007;33(11):1966–73.
- Vemuganti GK, Pasricha G, Sharma S, Garg P. Granulomatous inflammation in Acanthamoeba keratitis: an immunohistochemical study of five cases and review of literature. Indian J Med Microbiol. 2005;23(4):231–8.
- Motlagh BF. Recurrence of Acanthamoeba keratitis after deep anterior lamellar keratoplasty. Iran J Ophthalmol. 2014;26(1):53–7.
- Kim JS, Kim JC, Hahn TW, Park WC. Amniotic membrane transplantation in infectious corneal ulcer. Cornea. 2001;20(7):720–6.
- Casalita V, Sitompul R. Hasil Tata Laksana Transplantasi Membran Amnion pada Ulkus KorneaInfeksi di Departemen Ilmu Kesehatan Mata FKUI-RSCM Periode 2015–2017. Penelitian Deskriptif. Jakarta. Universitas Indonesia; 2017. Indonesian.
Copyright @ 2018 Authors. This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original author and source are properly cited.
mji.ui.ac.id